Case 1
- What is the diagnosis based on the blood test, and how is the diagnosis made?
- What additional blood tests are required?
- What are the clinical manifestations of this?
- What are the options / modes of delivery for treatment?
- Who is contraindicated for treatment?
- What tests are required prior to starting, and how often should they be monitored?
Case 2
- Who is this image of? What disease of the male organ did they describe?
- What is the progression of this disease?
- What are the key points in the history to aid management choices?
- Clinical assessment, diagnosis and investigations?
- What is the pathogenesis of this disease?
- What treatment options are there?
- What surgical options are available?
Spot Test: answers
Case 1
-
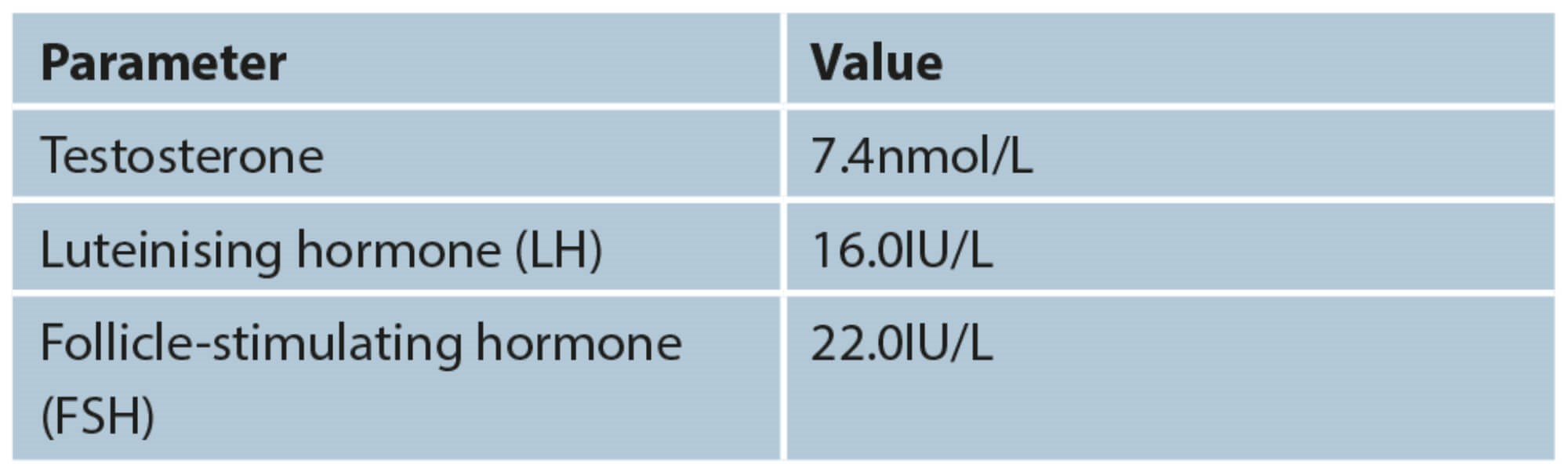
Low testosterone (T). T level lower than 8nmol/L based on two separate fasting blood levels obtained between 7am and 11am usually requires T therapy. Consider treatment when serum T levels are between 8-12nmol/l if they are symptomatic. Only treat if have combined low levels and are symptomatic.
-
Perform LH and FSH levels in conjunction with serum T levels, and add Prolactin levels if low serum T levels are detected. This will differentiate between primary and secondary forms of hypogonadism.
-
Low mood, erectile dysfunction / low libido, weight gain, decreased muscle mass.
-
Oral, injectable, and topical gel testosterone formulations.
-
Contraindications:
• Untreated prostate cancer: investigate an elevated serum prostate specific antigen (PSA)
• Male breast cancer
• Obstructive sleep apnoea
• Male infertility / desire to have children
• Haematocrit (Hct) >50%
• Severe lower urinary tract symptoms
• Severe chronic heart failure (New York Heart Association class IV)
• Not to be started <3/12 of a cardiac event
-
Assess and monitor treatment response at three months, six months and then yearly. Aim is T levels 15-33nmol/L. Monitor PSA, Hct (<0.54), liver and renal function.
Case 2
-
François Gigot de la Peyronie. He described Peyronie’s disease.
-
40% worsen, 47% stabilise and 13% improve.
-
To establish if in active or stable phase, presence of concurrent erectile dysfunction, ability to have penetrative intercourse, adequacy of penile length.
-
Examination of the organ for palpable plaque, photographs of the erect penis at three different angles. If unable to achieve erection artificial erection can be done to plan surgery in order to fully counsel the patient.
-
Precise cause unknown, but likely to be due to repeated micro-traumas to the tunica albuginea with abnormal wound healing. Transforming growth factor beta 1 (TGF-β) has been identified as a key growth factor involved.
-
Most drugs taken orally (e.g. phosphodiesterase-5 inhibitors such as tadalafil or non-steroidal anti-inflammatory drugs) or applied topically (e.g. verapamil, H-100 gel) either have not been tested in randomised controlled studies or have not been confirmed to be effective in placebo-controlled trials. Intralesion injections with collagenase and interferon a2b are supported by stronger evidence and are recommended in the European Association of Urology 2020 guidelines for men with stable disease, curvatures >30°, and seeking a non-surgical solution. Extracorporeal shock wave lithotripsy (ESWL) is another option currently being investigated. Traction devices show promise (even though there is limited evidence so far) but require extensive time applied.
-
Must be stable for three to six months before being considered and the patient should be counselled appropriately. There are three main types of surgical options for Peyronie’s: if the penile angulation is <60° with adequate penile length and rigidity then consider plication (tunical shortening procedure such as Nebit’s, Yachia, or pure plications); if >60° a tunical lengthening technique using a graft (e.g. Lue’s procedure) is an option; consider a penile prosthesis implant if there is severe wasting, erectile dysfunction or residual curvature.
Acknowledgement
Photo Credit: François Gigot de La Peyronie. Stipple engraving by Forestier after H. Rigaud. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0).




