Look out for part 2 of this series later in 2016 when the author will discuss settling into the research role of his fellowship and will reflect on his first year overseas.
This is the first in a series of articles that will aim to explore the benefits and challenges faced by trainees wanting to go on a fellowship. The series will look at the rationale for embarking on a fellowship, as well as reasons not to, timing of said fellowship, hoops that one might need to jump through and potential challenges encountered along the way. In addition, it will aim to share with the reader the personal challenges I faced in organising and going on my fellowship to Vancouver, based at the Vancouver Prostate Centre and University of British Columbia. Throughout the series, hopefully you will also gain an insight into what it is like to be on fellowship, including both the highs and lows.
So why go on a fellowship?
The reasons for wanting to go on a fellowship are multiple and individual. The word fellowship in itself means “sharing a community of interest” [1]. As such, in the context of medical practice, it usually represents a period of extended training within a predefined field. For some the reason to go on a fellowship will be the opportunity to experience another healthcare system, for others it will be to focus and concentrate on a subspecialty area of practice or research, and for others still it may be to gain extra experience in teaching, simulation or healthcare policy. Some will choose to go on a fellowship as they feel they are not ready to practise as a consultant and want extra time and training to feel comfortable with the significant leap from trainee to consultant. Moreover, perhaps there is often a perception that a fellowship will go some way to guarantee the consultant job of your choice. Whatever the reasoning behind it, it is paramount that before committing to such an undertaking you have a clearly defined set of objectives which you want to achieve.
My personal reasons for deciding to apply to go on a fellowship were a mixture of the above reasons. As I have an interest in healthcare management my decision to go was, at least in part, to experience first-hand what healthcare in an alternate country had to offer. I also felt it gave me a unique opportunity to spend two years as part of a world-renowned uro-oncology team with a year based in the laboratory doing pure research, followed by a year in the clinical domain. Whilst other, usually overseas, fellowships offer similar experiences they often come with the additional demand of further entrance exams (such as the USMLE) or for the need to source significant channels of funding – no mean feat in itself. Luckily, no such demands were placed on me. Again, these are all things that need to be considered when planning fellowships.
Timing is everything
For most trainees a fellowship will be undertaken either towards the end of their specialist training or following its completion. In part, this recognises the need for an adequate understanding of a speciality in general before aiming to undergo subspecialty training. After all, there is very little merit in trying to learn the intricacies of retroperitoneal lymph node dissection when you are still struggling to tie basic knots. That being said, other fellowships, such as simulation or education fellowships, might be taken at any time during higher specialist training. It is also worth noting, at this stage, the National Medical Director’s Clinical Fellow Scheme, sponsored by Professor Bruce Keogh and managed by the Faculty of Medical Leadership and Management. This scheme aims to support doctors in training to develop skills in medical leadership (visit www.fmlm.ac.uk/professional-development/national-medical-directors-clinical-fellow-scheme for more information).
One of the benefits of taking time out to go on a fellowship prior to Certificate of Completion of Training (CCT) is that upon return you will still have a job to come back to. This is a reason many trainees decide not to wait until after their CCT. This, however, may not continue to be the case; there is certainly, at least, a rumour that some surgical subspecialties may prevent those with training numbers from going on fellowship and argue that it should be the realm of the post-CCT trainee. However, as yet there is no specific published guidance to suggest this.
Time out of training – what is an OOP?
The Gold Guide for trainees [2] recognises a number of different mechanisms to spend time away from their speciality training programme. These include OOPE, OOPR, OOPT and OOPC. OOP stands for (time) ‘out of programme’ with E being for experience, R for research, T for training and C for a career break. All of these requests need prospective approval by the relevant postgraduate dean and trainees would normally need to have been in their training post for one year for approval. A full description of the ins and outs of the OOP regulations are beyond the scope of this article. However, it is important to note that any OOPT requires prospective approval by the General Medical Council (GMC), as well as the Specialist Advisory Committee (SAC) if it is to be counted towards CCT requirements. OOPR can also be counted towards time for CCT requirements, but again, only with prospective approval from the GMC, SAC and the deanery (Local Education and Training Boards).
Furthermore, once the GMC has approved these posts it remains for the SAC to confirm whether suitable training has been received during the post to satisfy curriculum requirements pursuant to the award of CCT. It is therefore important for anyone wishing to count their fellowship time towards their training to continue to keep their e-portfolio up-to-date.
Prospective approval – Deanery, SAC and GMC
Perhaps one of the most laborious parts of going on a fellowship is the paperwork. My advice for this is to start early; it can take up to six months to get all the paperwork together. The first thing to do is discuss your plans with your educational supervisor and get his / her support. Following this, a discussion with your training programme director (TPD) is imperative; they will then be able to point you in the right direction to the appropriate person at the deanery who should know what paperwork you are required to complete. This information is available on most deanery websites (see references 3 and 4 for examples).
This usually consists of an application form outlining the aims and objectives of the OOP with evidence of support from your educational supervisor and TPD, usually by signing the application form. This is then processed by the deanery who will ask the postgraduate dean to sign off on the OOP. Once the deanery has given approval you will also need to separately apply to the SAC either for prospective support for an OOPT or, in the case of any other OOP, a change to your CCT / Certificate of Eligibility for Specialist Registration (Combined Programmes) (CESR (CP)) date. The SAC usually require the following information:
- Exact dates of OOP
- Up-to-date CV
- Signed offer letter from the supervisor or medical staff with the exact dates of fellowship
- Letter of support or signed OOP form from your TPD including dates of OOP
- Confirmation that LETB / Deanery are aware of OOP
- Educational contract (which should include details of learning agreements and objectives)
- Timetable
- Job description
- Name and contact details of your supervisor.
Once both the deanery and SAC paperwork has been complete, the deanery will then apply directly to the GMC for prospective approval if you wish to count the time towards your training. At this point you should take heed of the following GMC guidance:
“The new GMC guidance on changes to the OOP process went live in April 2014. This guidance makes clear that all training must be prospectively approved if it is to count towards the award of a CCT or CESR (CP) and this is a requirement of the EU Directive. As of Monday 28 April 2014, the GMC will withdraw any application where the out of programme post has already started, regardless of the reason for it being submitted retrospectively.”
Once the deanery, SAC and GMC have approved the OOPT then you are ready to go. You are ready for the next onslaught of paperwork!
Where to go?
Depending on your reasons for going on a fellowship, the answer to this question could be anywhere. The Royal College of Surgeons of England (RCS) is currently seeking to ‘quality assure’ fellowships taken in England, Wales and NI [5]. There are a number of RCS approved urology-based fellowships available, which are worth considering. If you are looking to travel abroad one important consideration is language. This usually limits UK trainees to English-speaking fellowships. Australia and New Zealand are popular destinations, in part due to the similarities in training pathways to the UK; they also anecdotally are better remunerated than those taken in North America.
One of the other potential drawbacks of fellowships in the USA, as mentioned before, is the requirement to take the USMLE. This is, however, not a requirement in Canada. Therefore careful consideration should be taken to ensure you meet the qualifications required for whichever country or state you are considering, prior to applying for any fellowship. If research is important to you the types of programme on offer at your fellowship destination and potential qualifications are also important to think about. Other considerations include ease of obtaining visas and travel distance from home.
Getting there
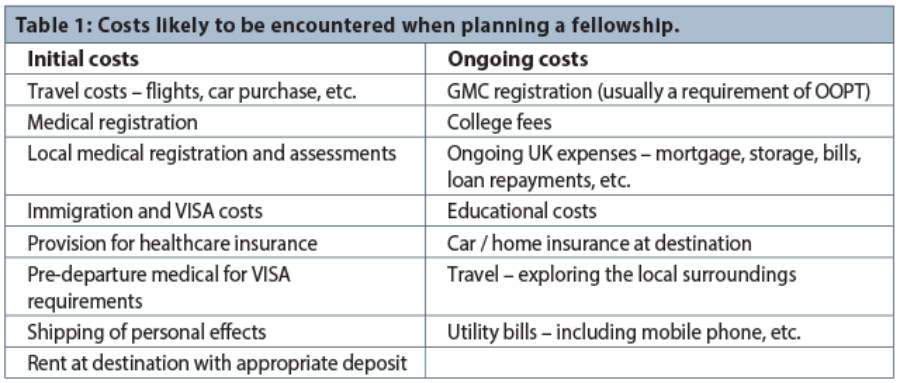
Once all the various approvals have been obtained the practicalities of going need to be considered. Even if that just means moving up the M6 corridor planning is important. If you have a family will they be coming with you? If you do not have a family are you planning to start one? If so what is the healthcare provision where you are going? You would be surprised by the number of international fellows expecting babies in my current institution! Will you be making a visit to the fellowship institution prior to starting either for an interview or to ‘suss the place out?’ How much will it all cost? What will I need? Table 1 below outlines some of the potential costs you might encounter. Although no published figures give details on the cost of going on a fellowship, anecdotal accounts suggest that you will need £10,000 to £15,000 to cover the initial costs you are likely to encounter.
Once you have answered all these questions, you will also need to remember to resign from your current post with adequate notice (if appropriate). You should also consider cancelling UK medical indemnity subscriptions and BMA memberships and decide what to do with your GMC registration; it is usually a stipulation for trainees to continue to pay to be both on the register and with a licence to practise as revalidation depends on this.
References
1. Oxford English Dictionary.
www.oed.com/view/Entry/
69110?rskey=QTjmbu&result=1#eid.
Accessed 11 September 2015.
2. Health Education England. A Reference Guide for Postgraduate Specialty Training in the UK. The Gold Guide, Fifth Edition, Version GG5. 2014.
http://specialtytraining.hee.nhs.uk/
files/2013/10/A-Reference-Guide-for-Postgraduate-
Specialty-Training-in-the-UK.pdf
Accessed 29 September 2015.
3. Health Education Wessex Out of Programme Experience.
www.wessexdeanery.nhs.uk/policies__
procedures/out_of_programme_experience.aspx
Accessed 20 October 2015.
4. Health Education Yorkshire and Humber OOP Policies.
www.yorksandhumberdeanery.nhs.uk/
pgmde/policies/training_policies/out_of_programme/
Accessed 20 October 2015.
5. Royal College of Surgeons of England National Fellowship Programme.
www.rcseng.ac.uk/surgeons/training/fellowships
Accessed 20 October 2015.
Declaration of competing interests: None declared.



