Introduction
Fournier’s gangrene (FG) is a rare but fulminant form of infective necrotising fasciitis affecting the perineum and external genitalia, which can rapidly progress along fascial planes. It most commonly affects men, but can occur in women and children, with a male to female ratio of 5:1 [1].
The French venereologist, Jean-Alfred Fournier gave the first clinical description of an idiopathic and rapidly progressive necrotising gangrene of the penis and scrotum, in an otherwise healthy young man in 1883 [2]. Although the condition is eponymously ascribed to him, Baurienne and Avicenna had described the same disease process earlier, in 1764 and 1877 respectively [3].
Furthermore, contrary to Fournier’s original description, subsequent experience has shown that rather than being idiopathic, in most cases FG has an identifiable cause (Box 1) and is commonly associated with several risk factors and / or co-morbidities (Box 2). Despite medical advances, FG continues to be associated with significant morbidity and mortality.
Box 1: Aetiology of Fournier’s gangrene
Urogenital
-
Urethral stricture +/- urine extravasation
-
Scrotal abscess
-
Epididymoorchitis
-
Indwelling catheter
-
Traumatic catheterisation
-
Hydrocele surgery / aspiration
-
Vasectomy
-
Circumcision
-
Prostate biopsy
-
Insertion of a penile prosthesis
-
Insertion of a TVT
-
Perineal trauma
-
Genital piercing
-
Delayed rupture of ileal neobladder
Anorectal
-
Perianal / ischiorectal abscess
-
Rectal biopsy
Anal dilatation
-
Haemorrhoidectomy
-
Rectosigmoid malignancy
-
Appendicitis
-
Diverticulitis
-
Strangulated inguinal hernias
-
Steroid enemas
Gynaecological
-
Infected Bartholin’s gland
-
Vulval abscess
-
Septic abortion
-
Episiotomy wound
-
Coital injury
-
Genital mutilation
Box 2: Comorbid risk factors for the development of Fournier’s gangrene
-
Diabetes (present in up to 60% of cases [4])
-
Chronic alcoholism (present in 25-50% of patients [7])
-
Extremes of age
-
Malignancy
-
Chronic steroid use
-
Cytotoxic chemotherapy
-
Radiation therapy
-
Lymphoproliferative diseases
-
Malnutrition
-
Morbid obesity
-
HIV infection
-
Chronic liver and kidney disease
-
Crohn’s disease
-
Suprapubic catheter
Aetiology and pathogenesis
FG has an identifiable cause in approximately 95% of cases [4,5]. Commonly, the necrotising process originates from an infection in the anorectum, urogenital tract or genital skin [6]. Trauma, recent surgery, urethral instrumentation, intramuscular injections, steroid enemas and the presence of foreign bodies have all been reported as causative factors [4]. In children, strangulated inguinal hernias, circumcision, omphalitis, insect bites, and burns have also been linked to the development of FG. Poor perineal hygiene and any condition associated with immunosupression may also predispose a patient to the development of FG.
Wound and / or tissue cultures from patients with FG typically demonstrate a polymicrobial infection of both aerobic and anaerobic organisms, with an average of four isolates per case [4]. Most of these are normal commensals in the perineum and genital areas, which opportunistically and synergistically become virulent and extremely destructive in patients with compromised immunity.
E coli is the predominant causative aerobe, and Bacteriodes species, the predominant anaerobe. Other commonly associated organisms include Proteus, Staphylococcus, Enterococcus, Streptococcus, Pseudomonas, Klebsiella, and Clostridium. The production of various endotoxins and enzymes including collagenase, heparinase and streptokinase by these organisms plays an important role in the pathological process; with platelet aggregation and complement reaction induced by aerobes, and heparinase and collagenase production by anaerobes, leading to microvascular thrombosis and skin necrosis. In addition, phagocytic activity in the necrosed tissues is impaired which further promotes spread of the infection [8]. Rates of fascial destruction as high as 2-3cm / hour have been reported [5,9,10].
Relevant anatomy
Understanding the anatomical relationship of the fascial layers, skin and subcutaneous structures in the perineum and abdominal wall, as well as the vascular supply in these regions, is key for any clinician treating the condition, not least because it has important implications for both the initial debridement, and subsequent reconstructive surgery.
The spread of infection is along the fascial planes, and is usually limited by the attachment of Colles’ fascia to the perineal body caudally and the clavicles cranially. For this reason, infection originating in the perineum or rectum can spread to involve the scrotum, penis and anterior abdominal wall right up to the level of the clavicles. However, whilst the superficial and deep fascia, and the skin (to varying degrees), are destroyed, the deeper muscular structures, corpora, urethra and cord structures are not usually involved unless they are the origin of infection. The testes are also usually spared as their blood supply originates intra-abdominally from the aorta. If the testes are involved it is usually a sign that the infection has originated or spread into the retroperitoneum. Involvement of the anal margin is also a key feature to assess on examination, in order to help determine the origin of infection (if it is not already clear from the history); anorectal sources of infection will usually start perianally and spread outwards, whereas urogenital infections tend to travel caudally along Bucks and Dartos fascia to involve Colles’ fascia, but will not normally spread to involve the anal margin because of restrictions posed by the attachment of Colles’ fascia to the perineal body.
The blood supply to the anterior abdominal wall and scrotal wall are also relevant; the inferior aspect of the anterior abdominal wall is supplied by branches from the inferior epigastric and deep circumflex iliac arteries, whereas branches of the external and internal pudendal arteries supply the scrotal wall. The internal pudendal artery (which supplies the posterior aspect of the scrotal wall) is the only one of these vessels which doesn’t travel within Camper’s fascia. Therefore, whilst all of the other vessels may become thrombosed in the pathogenesis of FG, thereby jeopardising the viability of the skin that they supply in the anterior scrotum and perineum, sparing of the internal pudendal artery often means that blood supply to the posterior aspect of the scrotal wall is preserved. This viable skin may then be used later in any reconstructive surgery.
Presentation
The clinical presentation of FG shows considerable heterogeneity. In some cases the onset and progression of disease will be insidious, starting with pruritis and discomfort in the external genitalia. In others, disease onset will be rapid with an immediately fulminant course. A high index of suspicion, particularly in those with relevant risk factors and co-morbidities is therefore needed if the condition is to be recognised and treated early.
Commonly, the infection will start as an area of cellulitis adjacent to the portal of entry of the infecting organisms. There may be significant swelling, but often with marked systemic signs and pain out of proportion to the physical findings. Crepitus of the inflamed tissues may be noted because of the presence of gas forming organisms [11]. A distinctive odour exhibited by the infected tissues and bronzing of the tissues are further characteristic features. As the condition and degree of inflammation and microvascular thrombosis within the subcutaneous tissues progresses, necrotic patches start appearing in the overlying skin, leading to extensive necrosis if untreated [12].
Investigations
FG is a urological emergency, and primarily a clinical diagnosis based on a thorough history and careful examination. Early diagnosis and treatment is key, and should not be delayed in the pursuit of obtaining further investigation results. Failing to treat the patient aggressively can rapidly lead to the development of sepsis with multi-organ failure – the main cause of death in these patients [13]. However, in cases where the presentation is atypical or where there is concern regarding the true extent of the disease, imaging modalities may have a role. Plain x-ray may show gas within the tissues whilst ultrasound may be useful to differentiate intrascrotal abnormality and might show a thickened gas-containing scrotal wall [14]. CT and MRI are useful in select cases to diagnose or exclude retroperitoneal or intra-abdominal pathology [15].
Other investigations are essential to identify co-morbid as well as causative factors. These include urinalysis, blood sugar measurements, appropriate bacterial evaluation of pus and / or tissue samples, full blood count, and renal and liver function blood tests.
The eventual need for further investigations such as cystoscopy, colonoscopy and biopsies may also arise in order to identify the source of sepsis.

Figure 1.
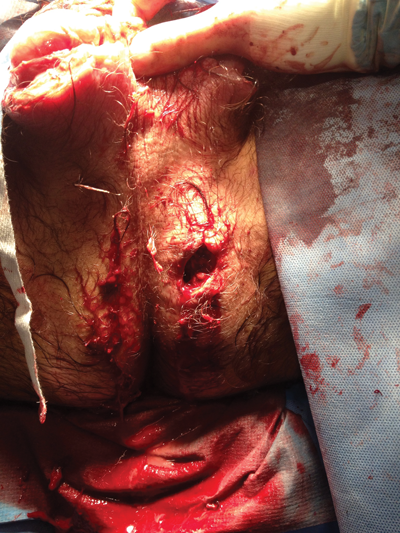
Figure 2.
Treatment and management
FG warrants an early, aggressive, multi-modal approach, which includes resuscitation and supportive care, broad-spectrum antibiotics, and early surgical debridement. One can argue, that of all these treatments, it is the latter which is most important; as if surgery is delayed there will be a negative impact on prognosis [16]. All non-viable, suspicious and necrotic tissue must be excised down to well-perfused bleeding tissue (see Figure 1 and 2). The areas of apparent cutaneous involvement data may be misleading in terms of the true extent of the subcutaneous disease below. Care must be taken not to inadvertently open up the deeper fascial planes, which can allow the infection to spread into fascial layers that were initially spared.
Initial antibiotic therapy should be broad spectrum to empirically cover all possible organisms but may then be rationalised once culture results and sensitivities are available. The usual combination includes a penicillin for the streptococcal species, a third generation cephalosporin, with or without an aminoglycoside for the gram-negative organisms, plus metronidazole for the anaerobes.
Urinary and / or faecal diversion may also be required depending on the original focus of the disease [11]. Re-look surgery is critical, and on average, 3.5 procedures are required per patient [17].
There is evidence to suggest the use of vacuum assisted closure (VAC) dressings may dramatically improve the speed of tissue healing and can minimise the size of residual skin defects [19]. Hyperbaric oxygen is also widely believed to be an effective adjunctive therapy in the treatment of FG. It is thought to neutralise anaerobic organisms and promote neutrophil function, fibroblast proliferation and angiogenesis [19]. However, there is little conclusive evidence regarding its effectiveness [20].
Depending on the extent of the skin defect after debridement and subsequent healing, further surgical reconstruction may be required to provide skin cover once the infection has resolved. Several techniques can be employed, including split skin grafts and myocutanous flaps. The testes may also require auto-transplantation (often into the inner thigh compartment).
Prognosis
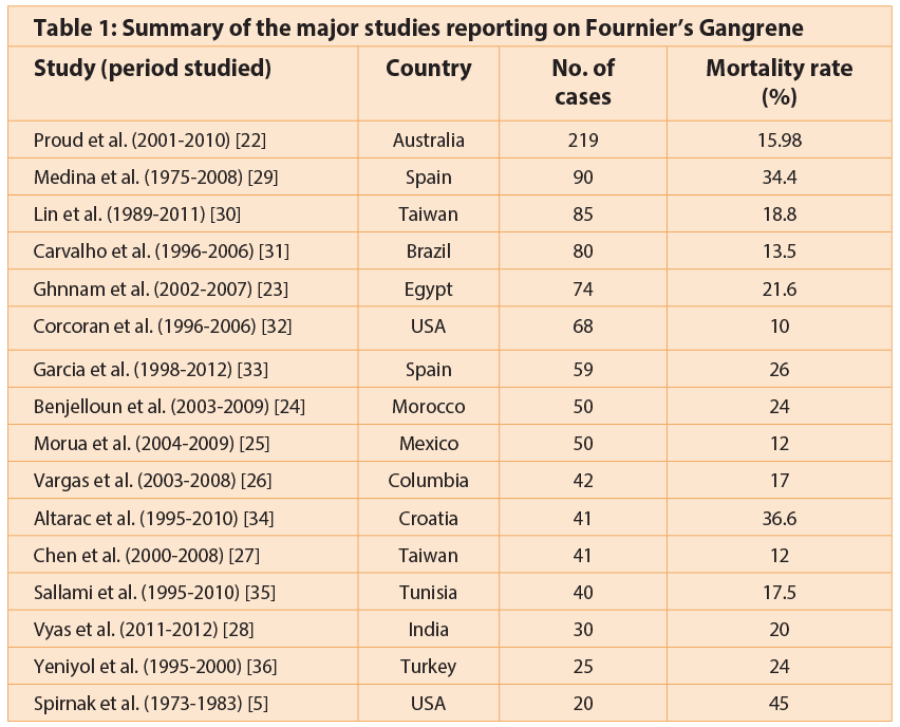
Early series reported high mortality rates with FG at around 80% [21]. More recent studies show an improvement with mortality rates generally less than 25% [22-28] (Table 1).
Factors that have been identified as negatively affecting survival include advancing age, primary anorectal source of infection, delay in treatment, extension of infection to the anterior abdominal wall, renal failure on admission, occurrence of septic shock, the need for postoperative mechanical ventilation, and immunocompromised states [24,37].
Fournier’s Gangrene Severity Index Score
The FGSI is based on deviation from reference ranges of the following clinical parameters:
-
Temperature
-
Heart rate
-
Respiratory rate
-
White blood cell count
-
Haematocrit
-
Serum sodium
-
Serum potassium
-
Serum creatinine
-
Serum bicarbonate
Each parameter is assigned a score between 0 to 4, with increasing values indicating greater deviation from normal. The sum of all the parameter values is then used as the final FGSI score.
Laor et al. [38] have developed a scoring system; the Fournier’s Gangrene Severity Index (FGSI), which may be used to quantify the severity of infection and help prognosticate the illness and predict mortality, using commonly measured vital signs and laboratory data. In this scoring system (Box 3), a score >9 was associated with a 75% probability of death, while a score <9 was associated with a 78% probability of survival [38].
In patients who do survive FG, morbidity rates can be high; long-term complications of the disease are not uncommon and may include chronic pain, chronic cellulitis and oedema, and impaired sexual function.
References
1. Ullah S, Khan M, Asad Ullah Jan M. Fournier’s gangrene: a dreadful disease. Surgeon 2009;7:138-42.
2. Fournier J-A. Gangrene foudroyante de la verge. Semaine Medicale 1883;3:345-8.
3. Nathan B. Fournier’s gangrene: a historical vignette. (Letter). Can J Surg 1998;41:72.
4. Eke N, Raphael J. Fournier’s Gangrene. In: Vitin A (Ed.). Gangrene - Current Concepts and Management Options. InTech; 2011.
5. Spirnak JP, Resnick MI, Hampel N, Persky L. Fournier’s gangrene: report of 20 patients. J Urol 1984;131:
289–91.
6. Mergenhange SE, Thonard JC, Scherp HW. Studies on synergistic infections. Experimental infections with anaerobic streptococci. J Infect Dis 1958;103:33-44.
7. Clayton MD, Fowler JE, Sharifi R, et al. Causes, presentation and survival of fifty-seven patients with necrotizing fasciitis of the male genitalia. Surg Gynecol Obstet 1990;170;49-55.
8. Smith GL, Bunker CB, Dineeen MD. Fournier’s gangrene. Br J Urol 1998;81:347-55.
9. Kilic A, Aksoy Y, Kilic L. Fournier’s gangrene: etiology, treatment, and complications. Ann Plast Surg 2001;47:523–7.
10. Sanchez-Mazzaferri F, Fadil-Iturralde J, Provenzal O, et al. Fournier’s gangrene. Our experience over 10 years. A review of the literature. Arch Esp Urol 1999;52:721-7.
11. Patty R, Smith AD. Gangrene and Fourniers gangrene. Urol Clin North Am 1992;19:149.
12. Laucks SS. Fournier’s gangrene. Surg Clin North Am 1994;74:1339-52.
13. Sutherland ME, Meyer AA. Necrotizing soft-tissue infections. Surg Clin North Am 1994;74:591-607.
14. Thwaini A, Khan A, Malik A, et al. Fournier’s gangrene and its emergency management. Postgrad Med 2006;82:516–19.
15. Amendola MA, Casillas J, Joseph R et al. Fournier’s gangrene: CT findings. Abdom Imaging 1994;19:471-4.
16. Elliott D, Kufera JA, Myers RA. The microbiology of necrotizing soft tissue infections. Am J Surg 2000;179:361-6.
17. Chawla SN, Gallop C, Mydlo JH. Fournier’s gangrene: an analysis of repeated surgical debridement. Eur Urol 2003;43:572-5.
18. Morykwas MJ, Argenta LC, Shelton-Brown E, et al. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg 1997;38:553-62.
19. Capelli-Schellpfeffer M, Gerber GS. The use of hyperbaric oxygen in urology. J Urol 1999;162:647-54.
20. Willy C, Rieger H, Vogt D. Hyperbaric oxygen therapy for necrotizing soft tissue infections: contra. Chirurg 2012;83:960-72.
21. Stephens BJ, Lathrop JC, Rice WT, et al. Fournier’s gangrene: historic (1764-1978) versus contemporary (1979-1988) differences in aetiology and clinical importance. Am Surg 1993;59:149-54.
22. Proud D, Bruscino RF, Holden D, Paul E et al. Are we getting necrotizing soft tissue infections right. A 10-year review. ANZ J Surg 2014;84:468-72.
23. Ghnnam WM. Fournier’s gangrene in Mansoura Egypt: a review of 74 cases. J Postgrad Med 2008;54(2):106-9.
24. Benjelloun el B, Souiki T, Yakla N, et al. Fournier’s gangrene: our experience with 50 patients and analysis of factors affecting mortality. World J Emerg Surg 2013;(8):13.
25. Morua AG, Lopez JA, Garcia JD, et al. Fournier’s gangrene: our experience in 5 years, bibliographic review and assessment of Fournier’s gangrene severity index. Arch Esp Urol 2009;62(7):532-40.
26. Vargas AH, Carbonell J, Osorio D, Garcia HA. Evaluation of Fournier’s necrosis in a high complexity hospital. Arch Esp Urol 2011;64(10):948-52.
27. Chen SY, Fu JP, Chen TM, Chen SG. Reconstruction of scrotal and perineal defects in Fournier’s gangrene. J Plast Reconstr Aesthet Surg 2001; 64(4): 528-34.
28. Vyas HG, Kumar A, Bhandari V, et al. Prospective evaluation of risk factors for mortality in patients of Fournier’s gangrene. A single centre experience. Indian J Urol 2013;29(3):161-5.
29. Medina Polo J, Tejido SA, de la Rosa Kehrmann F, et al. Fournier’s gangrene: evaluation of prognostic factors in 90 patients. Actas Urol Esp 2008;32(10):1024-30.
30. Lin TY, Ou CH, Tzai TS, et al. Validation and simplification of Fournier’s gangrene severity index. Int J Urol 2014;(7):696-701.
31. Carvalho JP, Hazan A, Cavalcanti AG, Favorito LA. Relation between the area affected by Fournier’s gangrene and the type of reconstructive surgery used. A study with 80 patients. Int Braz J Urol 2007;33(4):510-14.
32. Corcoran AT, Smaldone MC, Gibbons EP, et al. Validation of the Fournier’s gangrene severity index in a large contemporary series. J Urol 2008;180(3):944-8.
33. García Marín A, Turégano Fuentes F, Cuadrado Ayuso M, et al. Predictive factors for mortality in Fournier’ gangrene: A series of 59 cases. Cir Esp 2014; [Epub ahead of print].
34. Altarac S, Katušin D, Crnica S, et al. Fournier’s gangrene: etiology and outcome analysis of 41 patients. Urol Int 2012;88(3): 289-93.
35. Sallami S, Maalla R, Gammoudi A, et al. Fournier’s gangrene: what are the prognostic factors? Our experience with 40 patients. Tunis Med 2012;90(10):708-14.
36. Yeniyol CO, Suelozgen T, Arslan M, Ayder AR. Fournier’s gangrene: experience with 25 patients and use of Fournier’s gangrene severity index score. Urology 2004;64(2):218-22.
37. Martinelli G, Alessandrino EP, Bernasconi P, et al. Fournier’s gangrene: a clinical presentation of necrotizing fasciitis after bone marrow transplantation. Bone Marrow Transplant 1998;22:1023-6.
38. Laor E, Palmer TS, Tolia BM, et al. Outcome prediction in patients with Fournier’s Gangrene. J Urol 1995;154:89-92.
TAKE HOME MESSAGE
-
FG remains a life-threatening condition with high mortality rates.
-
Early diagnosis and multimodal treatment with surgical debridement, broad-spectrum antibiotics and good supportive care remain fundamental in the management of affected patients.
-
Proactive management of diabetic and immunocompromised patients with perineal infections is important to try and prevent development of FG.
Declaration of competing interests: None declared.





