Effective communication lies at the heart of specialist urological cancer care. For clinical nurse specialists and urology nurses, conversations often extend far beyond diagnosis and treatment, encompassing some of the most sensitive and life-changing discussions patients may ever face.
Whether supporting individuals through the delivery of difficult news, addressing concerns surrounding sexual function and intimacy, or helping patients navigate uncertainty and vulnerability, these nurses bring a unique combination of clinical expertise, empathy and experience to every interaction.
The insights shared in this article are drawn from interviews with experienced urology clinical and cancer nurse specialists: Deepa Leelamani, Sally Buttleman, Jessica Codling, Stephen Kinghorn and Dimitrina Baeva from Bart’s Health NHS Trust. Their daily practice requires not only advanced clinical knowledge, but also exceptional communication skills. Their reflections offer valuable perspectives on how sensitive conversations can be approached in ways that preserve dignity, foster openness, and support patients holistically throughout their care journey.
As a urology trainee or fellow, having these difficult conversations can be scary. Behind every procedure and every diagnosis is a patient navigating uncertainty, fear and often deeply personal concerns. Conversations around life-changing diagnoses such as cancer or sensitive issues like erectile dysfunction, can feel more daunting than the treatment itself. Unlike clinical knowledge, these communication skills can only be developed with observation, experience and sometimes – trial and error. It may be a challenging skill to develop but it should not be optional as it is paramount in providing the care our patient deserve.
To uncover the art of navigating these sensitive conversations, we spoke with five experienced Clinical Nurse Specialists (CNS) who have years of frontline experience under their belt. They offered practical insights into handling some of the most challenging conversations in urology and some tips on how we can start building these essential communication skills.
Identifying the “difficult” topics
What constitutes a difficult topic can be very personal to the practitioner and to the patient. We have all seen patients react differently to certain news. Some are comfortable to speak freely about their concerns whilst others will need astute observations to tease out that information. While many would assume cancer is the hardest topic, our CNS team highlights a range of other important challenges:
- Sexual health and erectile dysfunction (ED): Frequently cited as a primary challenge due to the social stigma and the profound impact on mental health and confidence.
- Lifestyle and behavioural change: Conversations around compliance with weight loss and exercise, as it requires a fundamental shift in patient behaviour.
- Social embarrassment: Addressing distress caused by Lower Urinary Tract Symptoms (LUTS), such as leaking or urgency, which can lead to social isolation and a loss of libido.
- Remote communication: Sensitive conversations are significantly more difficult over the telephone, as patients often do not feel “safe” to speak freely in a non-private environment.
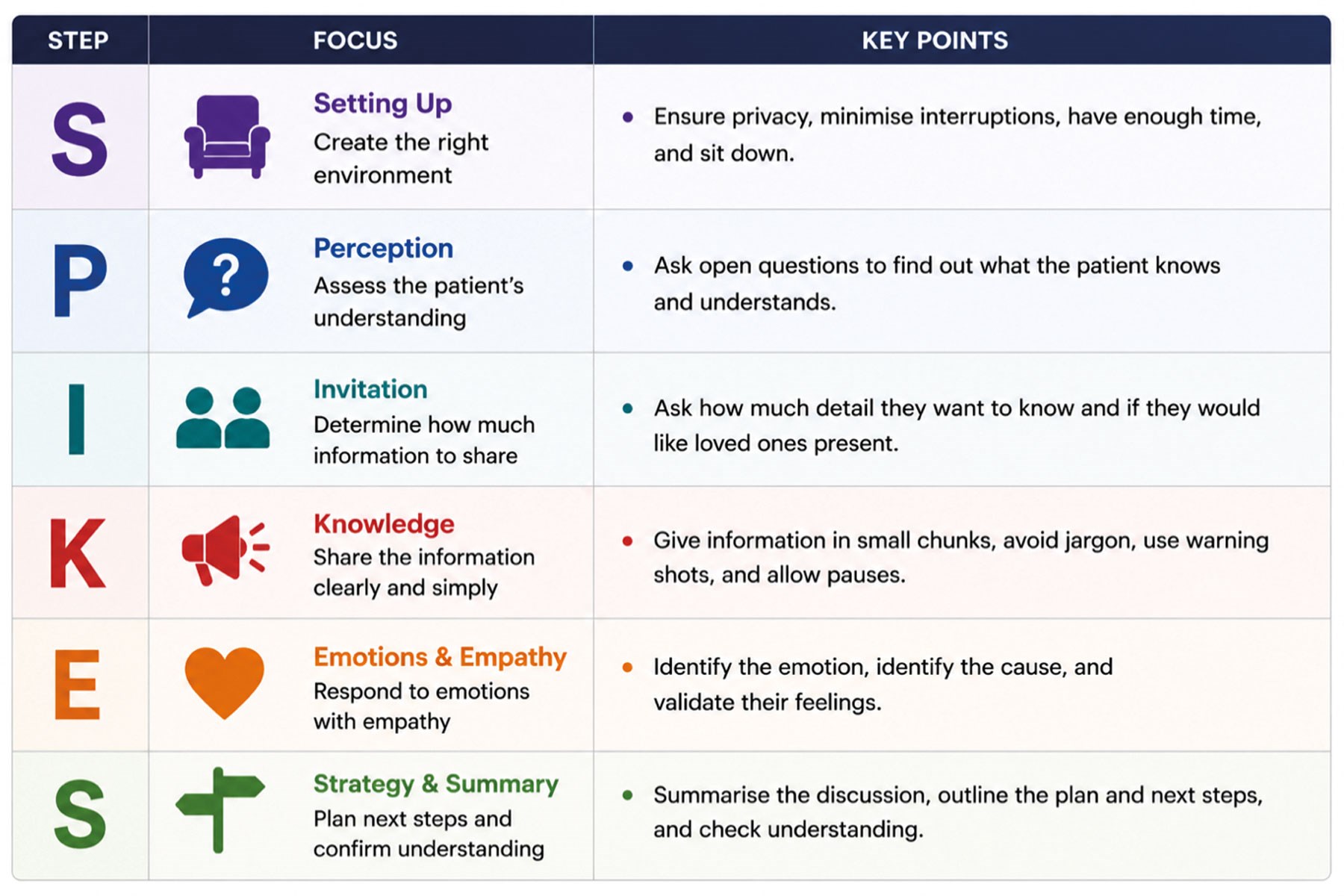
Figure 1.
Strategies for breaking bad news
Breaking bad news is one of the most difficult conversations to have. This skill has been assessed from medical school all through to the FRCS Urology examination. We have been taught about the SPIKES protocol (Figure 1) [1]. However, how can we utilise this in practice, tailor it to your patient and infuse it with empathy? Our CNS team recommended several key principles:
- Meticulous preparation: Prior to seeing the patient, it is of vital importance to read up on a patient’s full clinical history including scans, biopsies and previous notes. This gives us the ability to build on what they already know rather than starting afresh. This also instils confidence in your patients that you already know them even if you are meeting them for the first time.
- Clarity of plan: Have a firm grasp of the clinical plan before entering the room to avoid “muddying the water” or becoming flustered during the conversation. If you do not know the answer to their question, it is always better to be honest and find out or clarify before answering.
- Emotional boundaries: Remind yourself that you do not need to “fix” the patient’s feelings; acknowledging distress is often more powerful than trying to resolve it.
- Gauging information needs: To provide a powerful conversation, tailor your consultation by assessing a patient’s level of understanding and how much information they are ready to receive in a single sitting.
Navigating the “elephant in the room”: Sexual health
Urology involves discussion about highly sensitive body parts and the function of said body parts. This is usually a very private aspect of a patient’s life and is sometimes rarely shared with even family and close friends. Nonetheless, as urology practitioners, it is important to break the taboo and address these issues with them. Our CNS team uses normalised language to help break down barriers.
- Holistic approach: It is important for clinicians to approach and assess each patient’s individual sexual identity and needs. It is crucial not to make assumptions and provide patient’s a safe and non-judgemental space for consultations.
- Normalising embarrassment: Reassure patients that, whilst the topic may feel sensitive for them, it is a routine and clinical part of the practitioner’s work. Emphasising that it is a universal problem can make patients feel less isolated in their experience.
- Safe space: Having a safe physical environment can help patients open up. They have noted that face-to-face consultations are often more effective than telephone calls, as the simple act of “closing the door” helps signal a protected and confidential space.
- Involving the partner: The team also agrees that involving partners can be vital, as these issues are often shared experiences. Nonetheless, always check with the patient first, in order to respect their privacy and cultural values [2].
Managing distress and conflict
When having difficult conversations, it is hard to predict how a patient or their family is going to react. Sometimes, when given bad news, it triggers their threat response that disrupts their sense of fairness, safety and control [3]. When faced with distressing information, the brain’s amygdala is activated, which can cause people to react emotionally rather than rationally [4]. The healthcare professional can help by acting as a stabilising pillar of support for both the patient and the family.
- Validating emotions: Acknowledging the distress directly can often help the patient feel heard and de-escalates tension. For example, saying “I can see that you are very distressed.”
- Calm composure: Maintaining a calm composure as a practitioner can help patients find a safe emotional space to mirror.
- The power of silence: Be brave enough to tolerate silence and know when not to speak.
- Focusing on what can be done: Shift attention toward actionable support, highlighting that even in disease progression there is always scope for symptom control, quality of life improvement, and ongoing care and reassurance.
Useful “go-to” phrases
Having some effective “go-to” phrases that have been tried and tested can help with the flow of a conversation and sometimes, a spring-board for the next segment of the consultation. It is however important to recognise that these phrases should be tailored to your own communication style lest it comes across scripted. Observations of others conversation can provide inspiration on what works. Our CNS team recommends:
- Beginning consultations with a focused check-in such as “What is your main concern today?” ensuring that the patient’s priorities are identified early.
- Clarity can be improved by using accessible terms like “waterworks” or “leakage” instead of complex medical jargon.
- Maintain shared decision-making by asking permission before progressing, for example: “Is it okay if we talk about the next steps now?”
- Validating the patient’s emotional response with phrases such as “It’s completely normal to feel this way” helps normalise distress and build trust.
Practical tips: What not to say
The nuances of what not to say is difficult to pin down. Sometimes, even well-intentioned phrases can unintentionally be dismissive or offensive to certain individuals. For example, saying “I know how you feel,” can be mentioned in a bid to establish rapport and express empathy but this may be misconstrued to be patronising and untrue for certain patients. If they are distressed by a cancer diagnosis for example, they may challenge that you as a healthcare practitioner will never ‘know’ how they feel.
Reassurances like “everything will be fine” may feel empty when uncertainty exists. Comments such as “don’t cry” can suppress emotional expression rather than support it.
Ultimately, certain phrases may work well on some but terribly on others. Patients need to be supported in different ways and during your consultation, you are also trying to ascertain how best you can do that. If your heart is in the right place and your intentions are well-intended, you do not have to panic if a certain phrase or wording did not land right. You can acknowledge, apologise and try again.
TAKE HOME MESSAGES
The overarching theme from the Barts Health team is that communication is a skill that is never “finished” and requires constant refinement. Reflection is key. If a consultation goes poorly, do not be discouraged; instead, ask yourself what could be improved. You can watch others and have others watch you. The constant cycle of wanting to do better is what drives us to provide the best care our patients deserve.
References
1. Baile WF, Buckman R, Lenzi R, et al. SPIKES – A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302–311.
2. General Medical Council. Confidentiality: good practice in handling patient information. GMC 2017.
www.gmc-uk.org/ethical-guidance/ethical
-guidance-for-doctors/confidentiality
[Last accessed May 2026].
3. Rock D. SCARF: a brain-based model for collaborating with and influencing others. NeuroLeadership J 2008;1:44–59.
4. Goleman D. Emotional intelligence: why it can matter more than IQ. New York: Bantam Books; 1995.







