In this series of articles I am going to show you some of the exhibits contained in the Museum of Urology, hosted on the BAUS website (www.baus.org.uk).
In the last article I said I would write about another old urological instrument recently acquired for the Museum of Urology; one, that until recently, I had never heard of. I am joined this month by Pravisha Ravindra, a urology trainee who was also intrigued by this unusual instrument and was as surprised as I was to find out it was not abandoned from clinical practice that long ago.
While the development of the urethroscope and the cystoscope are inextricably linked, the two procedures of urethroscopy and cystoscopy were, historically, quite separate. It was recommended that urethroscopy was carried out a day or two before the cystoscopy in case any obstruction was encountered. JAB Macalpine warned that the areo-urethroscope should never be employed immediately following a failed cystoscopy due to the risk of fatal air embolism. So, although we examine the urethra immediately prior to entering the bladder with our modern cystoscopes, in the past completely separate cystoscopes and urethroscopes were developed. What we use now would, from about the 1920s, be termed a panendoscope, capable of doing both.

Figure 1: The Holborn aero-urethroscope.
The principle of using air insufflation to visualise and treat diseases of the urethra gave rise to the device known as the aero-urethroscope (Figure 1). We are so used to using fluid in endourology, this may appear a little alien; imagine a small rigid sigmoidoscope for use in the urethra.
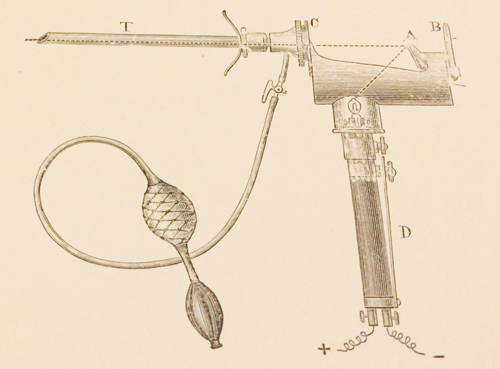
Figure 2: A Geza von Antal aero-urethroscope.
The earliest identifiable report of using air-inflation in male urethroscopy was by Geza Von Antal of Budapest in 1887 (Figure 2). He was the first professor of the first urological hospital in Hungary – it had 20 beds. He was also the author of the first Hungarian textbook on genito-urinary disease in 1888. The instrument used was a modified Grunfield urethroscope using an external light source and head mirror to reflect illumination down the scope. It was designed to separate and distend all the urethral walls so that all inflated portions could be inspected at the same time, “with a sensation that was not disagreeable to the patient”. Karel Pawlik, a Czech gynaecologist, had utilised an analogous device for visualising the female urethra a year previously. In 1890, Frank Hewell Jr described a similar instrument followed by Howard Kelly who was influential in establishing the device (and aero-cystoscopy) in America.
Hurry Fenwick from The London Hospital modified a Leiter instrument to identify retention cysts of Cowper’s glands as a cause of urethral stricture. He also used the device to treat membranous and large caliber strictures. However, critics of the Fenwick device described it as cumbersome. Wyndham Powell also based his design on the Leiter scope.
George Luys in 1902 added a magnifying lens to the end as this allowed any urethral lesions to be examined in greater detail, and continued to use his device even after the First World War.
Branford Lewis and Ernest Mark, both American professors of genito-urinary surgery, presented a Fenwick device with suitable improvements in the Journal of the American Medical Association in 1903. They felt that air distension was much better than water distension when it came to urethral visualisation and the best patient position was recumbent. While recognising that preliminary cocainisation of the urethra may be necessary for some patients to permit the procedure, they recommended that it should be avoided as mucosal changes may result. Lewis and Mark authored Cystoscopy and Urethroscopy for General Practioners detailing findings in a normal and diseased urethra.
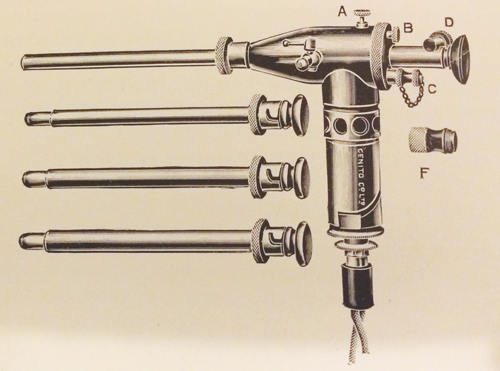
Figure 3: Swift Joly aero-urethroscope.
In 1914 John Swift Joly of St Peter’s, London published in The Lancet ‘An operating and observation urethroscope’ which he himself had designed. He described a probe, knife, curette, electrolysis needle and electric cautery working element options. India-rubber cones were used to create an airtight seal. Swift Joly promoted his instrument as simple, durable and providing effective and ergonomic illumination. It was updated in 1921 (Figure 3).
Archibald Cambell, Medical Officer at the Portsmouth Venereal Clinic, was particularly appreciative of the device as it allowed ‘general use’ in the community, and was not just in the armamentarium of specialists in London or the provincial teaching centres. His thoughts on how the weight of the Wyndham Powell device was obstructing easy use were published in The Lancet in 1918. He described his own modifications to the Luys’ side channel device, which included a lamp holder and removable lenses (so that the instrument could be sterilised by boiling).

Figure 4: The Holborn aero-urethroscope, cased.
In 1922 Wyndham Powell updated his device, which appeared in the catalogue of John Weiss and Son Ltd. It was described as, by far the most satisfactory and least irritating method of examining the anterior urethra and treating its diseases. For the price of £6, the aero-urethroscope came with double bellows, obturator, five urethral tubes (of varying size) and spare lamps. The Holborn aero-urethroscope won the Grand Prix and Gold medal at the 1913 London Medical Congress. The instrument we have in the Museum of Urology is a Holborn scope (Figure 1 and 4).
Although cystoscopy was felt to be a specialist procedure, indeed it almost defined the new speciality of urology, urethroscopy was deemed to be suitable for non-specialists such as general practitioners and venereologists. Harkness, writing on urethritis moaned that, “If all venereologists were skilled in using the anterior urethroscope urethral strictures would rarely follow gonorrhoea or non-gonococcal urethritis”.
Despite the introduction of irrigation fluid for cystoscopy air appeared to be a useful and comfortable medium to distend the urethra for maximal visualisation, urologists and non-specialists continued to use aero-urethroscopy as a separate distinct method for many years after the abandonment of air cystoscopy, remaining in use into at least the 1950s. In fact Harkness, quoted above was writing in 1950 and included a chapter on the use of the aero-urethroscope; he favoured the Swift Joly model.
So, the urethroscope was quite different to the cystoscope of the specialist urologist. The prolonged use of air meant no bottles of irrigation fluid were needed, it could be kept in a GU clinic or carried in a GPs bag. I suspect that these aero-urethroscopes were in use in GU clinics and consulting rooms well within living memory of some recently retired doctors and sisters.
Next time, I’ll be writing on a topic with a Scottish theme, looking forward to BAUS 2017 in Glasgow.




