Epidemiology
Partial segmental thrombosis of the corpus cavernosum (PSTCC) is a rare condition and usually presents in young men. Approximately 56 cases have been reported in 34 publications since 1976, when the first two cases were described [1,2]. The mean age of presentation is 31 years old (range 18-59 years).
Pathogenesis
In earlier case reports where surgical exploration was the preferred management for ongoing penile pain, a distinct fibrous septum was found within the corpus cavernosum separating the proximal part of the thrombus from the uninvolved corpus cavernosum. Ilicki et al. suggested a two-hit theory in which a transverse membrane divides the corpora into a proximal and distal portion and a second triggering event such as microtrauma predisposes the individual to developing PSTCC [3]. This theory has again been highlighted in the recent largest European case series published by Weyne et al. [4].
Risk factors associated with PSTCC are: haematological abnormalities (thrombophilia, sickle-cell disease), alcohol abuse or drugs (cocaine, marijuana), hypercoagulability associated with dehydration, surgery, malignancy, long-distance flights, as well as microtrauma following vigorous sexual activity or prolonged cycling [3-5].
Clinical presentation
The most common symptoms are perineal and penile pain with a distinct perineal swelling. It almost always occurs unilaterally and must be differentiated from a low flow priapism if the penis remains tumescent. PSTCC has been described as a partial priapism although a prolonged and painful erection is not always present. Painful erections and erectile dysfunction have also been reported but most symptoms improve within three to six months of conservative treatment [3-5].
On examination, the penis can appear semi-erect depending on the position of the thrombus and a lump can be felt on the affected side of the penile shaft or within the perineum [3-5].
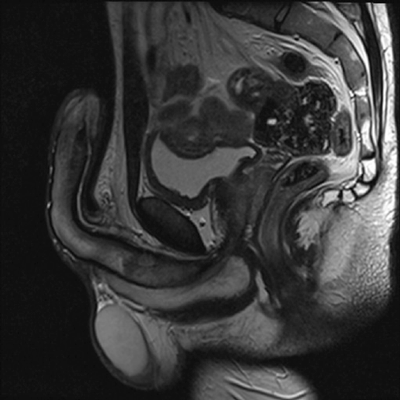
T1w-MRI (Sagittal) post IV contrast with no enhancement of right corpus cavernosum thrombus.
Investigations
It is important to establish the diagnosis promptly when patients present with perineal pain and a palpable mass. An inflammatory mass or malignancy can be excluded by undertaking cross sectional imaging with either CT or MRI [6-8].
MRI (see figure below), contrast-enhanced ultrasound (CEUS) or ultrasound doppler (USS) can be used to confirm the presence of the thrombus within the corpus cavernosum, as a well-defined non-enhancing mass [5,8-12]. Although CEUS is cheaper than performing serial MRI imaging, it is operator dependent [5].
All patients should undergo routine blood tests and thrombophilia screening on presentation.
Management
Although this condition has previously been treated either with needle aspiration of the thrombus or open surgical evacuation, the recommended treatment is conservative with systemic anticoagulation, either with low molecular weight heparin, aspirin or oral anticoagulants [3-5,13,14]. However, in patients suffering significant pain despite maximum analgesia, surgical evacuation of the thrombus can be performed [4].
Most patients maintain their erectile function without the need for PDE5-i for more than six months but follow-up serial MRI imaging is advised to check for resolution. Anticoagulation treatment is not required for more than six months, however due to the rarity of this condition, this is only based on previous reported cases and the recurrence rate is unknown.
Conclusion
Segmental thrombosis of the corpus cavernosum has a characteristic appearance on MRI and should be suspected in men presenting with acute perineal pain associated with a palpable penile shaft mass or perineal mass with or without a prolonged erection. The thrombus size appears to reduce after three months of anticoagulant or antiplatelet treatment and erectile function improves gradually within six months without the need for ongoing pharmacotherapies. However, long-term outcomes are unknown and larger case series are required to establish a unified practice in the management of this condition.
References
1. Hillis RS, Weems WL. Priapism: an unusual presentation. J Urol 1976;116:124–5.
2. Gottesman JE. Recurrent partial priapism.
Urology 1976;7(5):519-20.
3. Ilicki J, Krauss W, Anderson S-O. Partial segmental thrombosis of the corpus cavernosum: a case
report and a review of the literature.
Urology 2012;79:708-12.
4. Weyne E, Schillebeeck C, Jamaer C, et al. Idiopathic partial thrombosis (IPT) of the corpus cavernosum: a hypothesis-generating case series and review of the literature. J Sex Med 2015;12:2118–25.
5. Sauer S, Goltz JP, Gassenmaier T, et al. Partial segmental thrombosis of the corpus cavernosum (PSTCC) diagnosed by contrast-enhanced ultrasound: a case report. BMC Urolology 2014;14:100.
6. Gentile G, Broccoli A, Brunocilla E, et al. An isolated penile mass in a young adult turned out to be a primary marginal zone lymphoma of the penis. A case report and a review of literature. Anticancer Res 2013;33:2639-42.
7. Burkhalter JL, Morano JU. Partial priapism: The role of CT in its diagnosis. Radiology 1985;156:159
8. Asbacha P, Oelrich B, Haasec O, et al. Acute partial segmental thrombosis of the corpus cavernosum: imaging findings on ultrasound, computed tomography, and magnetic resonance imaging.
Clin Imag 2008;32:400–2.
9. Pegios W, Rausch M, Balzer JO, et al. MRI and color-coded duplex sonography: diagnosis of partial priapism. Eur Radiol 2002;12:2532–5.
10. Kimball DA, Yuh WT, Farner RM. MR diagnosis of penile thrombosis. J Comput Assist Tomogr 1988;12:604-7.
11. Machtens SA, Kuczyk MA, Becker AJ, et al. Partial Unilateral penile thrombosis: Magnetic resonance imaging and management. J Urol 1998;160:494-5.
12. Galvin SD, Letts JA, Sampangi NR. Magnetic resonance imaging of partial segmental priapism (segmental thrombosis of corpus cavernosum). Urology 2009;73:275-6.
13. Lewis JH, Javidan J, Keoleian CM, et al. Management of partial segmental priapism. Urology 2001;57:169.
14. Goeman L, Joniau S, Oyen R, et al. Idiopathic partial thrombosis of the corpus cavernosum: conservative management is effective and possible. Eur Urol 2003;44:119-23.
Acknowledgement
Photos are used with patient consent.
TAKE HOME MESSAGE
-
Segmental thrombosis of the corpus cavernosum is rare, but should be suspected when patients present with the characcteristic symptoms and referred for a specialist opinion.
-
MRI of the penis / pelvis will identify thrombus within the corpus cavernosum which unlike malignant lesions appears smooth with no contrast enhancement.
-
Patients should be treated for at least six months with anticoagulants and the thrombus is expected to resolve with improvement in both perineal pain and erectile function.


