In the third article in this series the authors describe their experience with the very rare indications for laparoscopic stone surgery.
Case 1
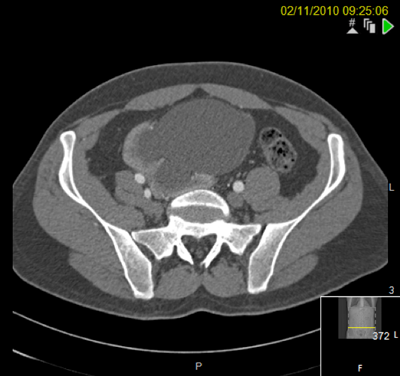
A 44-year-old woman presented with several months of malaise and right flank pain. A CT scan demonstrated a 26 x 25mm upper pole calyceal stone with an adjacent abscess that had perforated the capsule and some adjacent atelectasis. She was transferred from a referring hospital and treated with antibiotics and re-imaged.
Percutaneous nephrolithotomy (PCNL) failed. Although the calyx was successfully punctured, due to the lack of overlying cortex, no track could be established.
The patient underwent a laparoscopic nephrolithotomy. A right-sided four-port transperitoneal approach was used. The upper pole was extremely stuck and scarred and identifying the stone was very prolonged and difficult despite intraoperative fluoroscopy.
The upper pole was incised, the stone delivered and the calyx closed with 3-O PDS. A retrograde examination at three months revealed no leak.
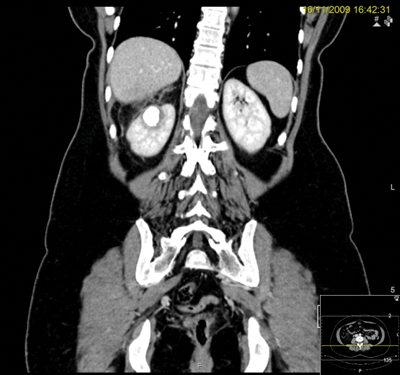
CT scan.

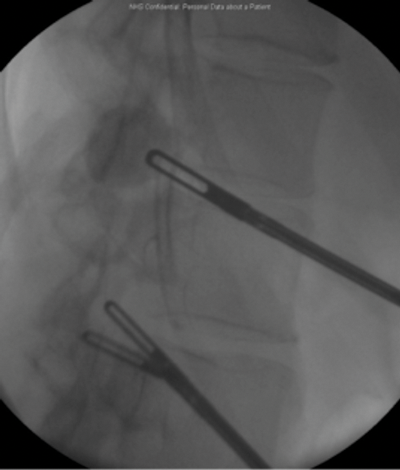
Marking for PCNL access.
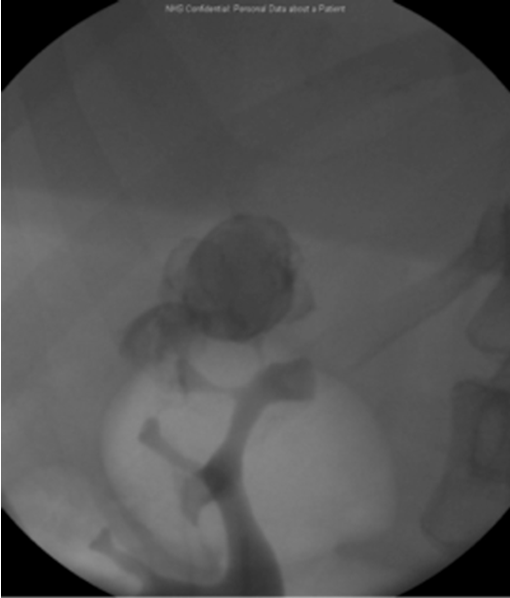
Pre-laparoscopy retrograde examination.
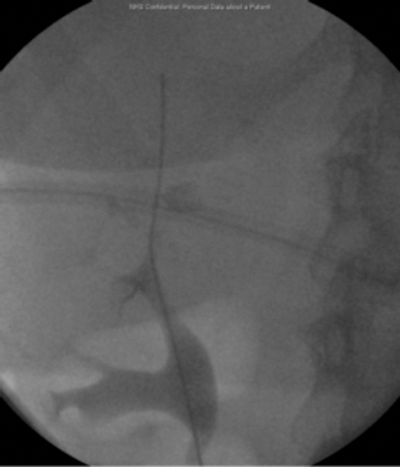
Intraoperative fluoroscopy used to identify the stone.
Three months postoperative.
Learning points
-
This is a rarely performed operation with limited indications and the patient questioned why it had not been performed as a primary procedure.
-
Do not presume stone identification will be straightforward.
-
Utilise intraoperative ultrasound.
Case 2
A 37-year-old male presented with stones in a right pelvic kidney. Flexible ureteroscopy demonstrated a tight and very tortuous ureter with no access to the renal pelvis.
PCNL was discussed at a specialist x-ray meeting but considered unsafe due to the risk of perforating overlying bowel.
A right sided transperitoneal laparoscopic approach was utilised, sweeping ascending colon medially. The renal pelvis was incised and stones were removed using a flexible cystoscope and the renal pelvis was closed over a stent.
At three years postoperatively, the patient was asymptomatic with stable renographic function and stone-free.

Figures above demonstrate worsening hydronephrosis preoperatively.

The patient postoperatively.
Case 3
A 59-year-old woman with a right-sided duplex ureter presented with right flank pain and confirmed recurrent urinary tract infection and a right lower pole calculus lying peripherally with very little overlying cortex.
PCNL was considered but a laparoscopic approach was preferred due to the radiological lack of overlying cortex. A four-port retroperitoneal laparoscopic approach was utilised.
The stone was identified in the lower pole and extracted via a nephrotomy incision but fell into the retroperitoneum and could not be found. The lower pole cortex was closed over with 3-O interrupted PDS sutures and a 20 Robinson’s drain placed into the retroperitoneum.
The patient is pain free with no further urinary tract infections postoperatively. The stone is still visible in the retroperitoneum on CT scanning but has caused no further problems 10 years on from surgery.

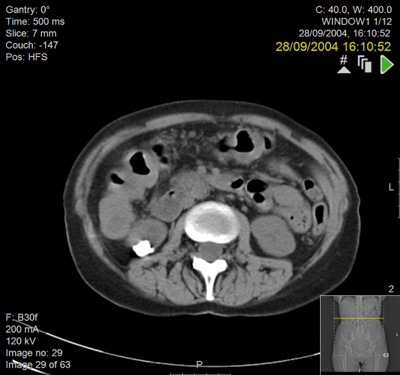
Preoperative IVU and CT demonstrating very little overlying renal cortex in duplex system.
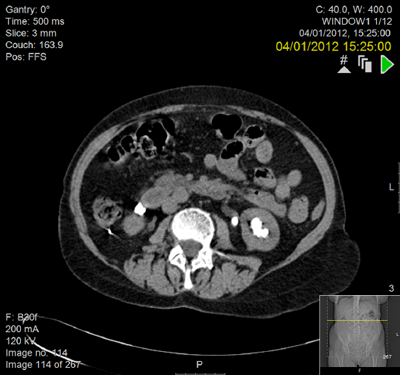

Seven years postoperatively. New left staghorn calculus and right-sided fragment demonstrated outside the kidney.
TAKE HOME MESSAGE
-
These cases are unusual and amount to only three examples in combined consultant practice of 26 years across two large centres.
-
Despite advances in endourological techniques not all stones can be successfully treated in this way.
-
Laparoscopic or robotic approaches to these rare and difficult cases should only be performed in experienced laparoscopic / robotic centres.
-
Intraoperative imaging is essential for stone localisation.




