One of the most interesting aspects of attending international meetings is the rare but invaluable, honest presentation of complex cases. We aim to present the readers with some complex and challenging ongoing cases in endourology.
Case 1
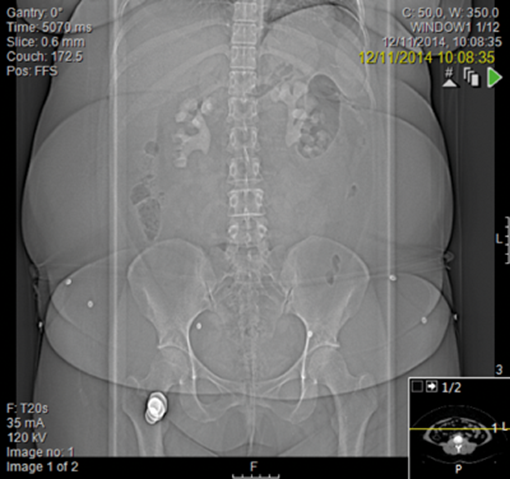
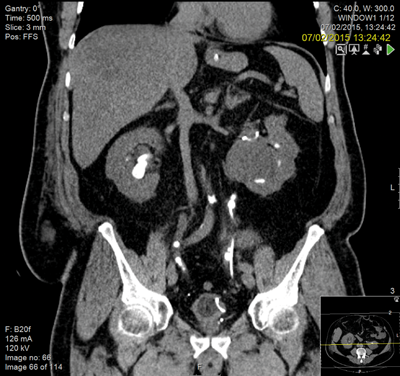
A general practitioner ultrasound was performed on a 29-year-old woman which hinted at bilateral stones. She gave a history of urinary tract infections throughout her pregnancy but had no paediatric history of note. She weighed 105kg with a body mass index (BMI) of 43 and was chronically anaemic with a haemoglobin of 97 and a creatinine of 186 and urine colonised with E. coli.
Management
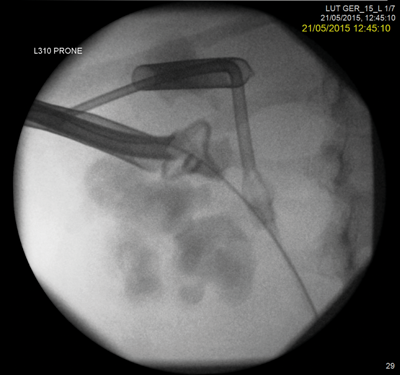
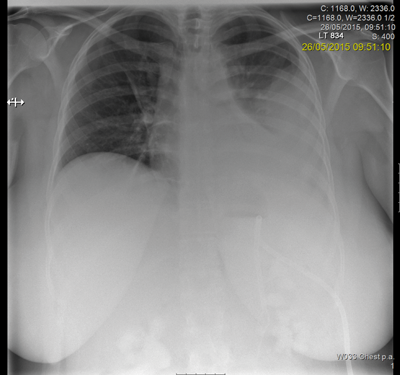
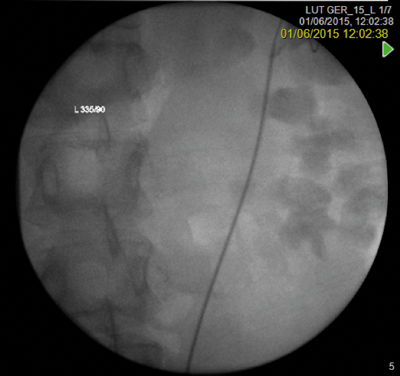
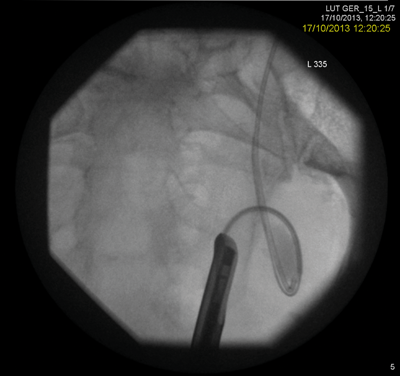
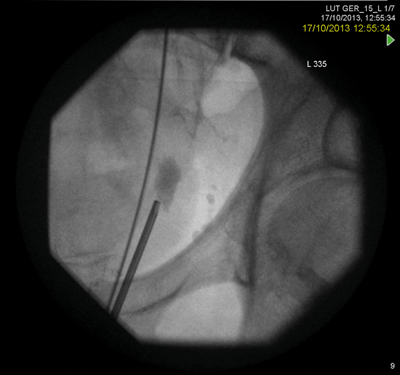
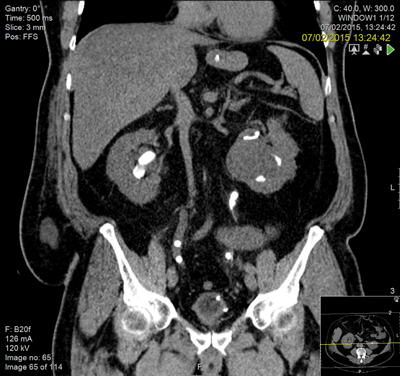
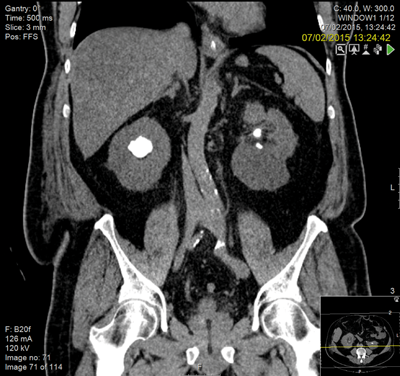
Following discussion at an X-ray meeting and a nephrology opinion, a left-sided percutaneous nephrolithotomy (PCNL) was performed in the prone position. Two tracts were placed by the urologist into the mid and upper portion of the kidney, clearing a reasonable volume and the patient was left with two nephrostomy tubes. The patient developed a postoperative reactive pleural effusion and chest infection requiring a chest drain. A prone CT revealed no radiological evidence of a pleural injury.
She was discharged with a double pig-tail stent which was sited retrogradely with no anaesthetic or sedation and was well tolerated.
Discussion
The lower pole is my concern. She has a degree of infundibular stenosis exiting the upper pole and indeed entering the lower pole, with poly-calyceal disease. She already has cortical thinning and will require many percutaneous punctures to clear her of stones on the left side. At the end of this, of course, she may be left with very little residual function. We are then faced with the right kidney. I requested a second opinion from a London teaching hospital and no change in management was suggested.
Learning points
- What is the end state with this patient? Probable renal replacement therapy.
- Retrograde stent placement with no anaesthetic or sedation is a useful technique.
- Prone CT is useful for imaging the pleura in the postoperative phase.
- Morbid obesity is now an accepted part of treating stone disease. In female patients the subcutaneous adipose tissue often falls to one side in the prone position.
- A second opinion from an expert in the field is not an admission of failure but a confirmation of safe practice.
Case 2
A known male stone former with significant cardiovascular co-morbidity and a history of a low anterior resection history presented with a large left lower ureteric stone having undergone a failed ureteroscopy by another surgeon with resection of the ureteric orifice.

A rendezvous procedure was performed in the supine oblique position. The radiologist punctured the non-dilated kidney, feeding a wire antegradely to the bladder, allowing subsequent ureteroscopy and stone clearance.
Learning point
Multiple failed attempts at ureteroscopic or percutaneous access do not help the doctor-patient relationship and can potentially put the patient at unnecessary risk when comorbidity is present. The Rendezvous procedure should not be forgotten as a ‘one stop’ method of dealing with ureteric obstruction. A combined antegrade and retrograde approach may decrease the number of separate interventions required to successfully cross a difficult stricture.
Case 3
A 57-year-old male was transferred from a referring hospital with deteriorating renal function (creatinine 830). He had a laparostomy secondary to ischaemic colitis and a partial right staghorn calculus, bilateral ureteric stones and numerous stones within his left kidney. He was obese, diabetic and had a previous myocardial infarction with a right-sided stoma and an open abdominal wound, secondary to a hemi-colectomy.
Following resuscitation with a right nephrostomy, he underwent bilateral ureteroscopy and was left with bilateral stents and small fragments adjacent to the ureteric stent.
Learning points
- The relationship between ischaemic colitis, prolonged immobility and stone disease.
- The possible need for supine PCNL in this case and the requirement for such cases to undergo surgery in hospitals with a high throughput of PCNL.
- The high chance of a postoperative ileus in this case.
- Recurrent stones are expected as are postoperative complications in a patient such as this. Consent is the key to managing patient expectations.




