Case 1
- What does this x-ray of the kidney, ureter and bladder (KUB) show?
- What are the likely causes?
- What is the pathology behind medullary sponge kidneys (MSK)?
- What is the risk of urolithiasis with MSK?
- How are such patients treated?
- What is the long-term prognosis?

Case 2
The patient from Case 1 presents as an emergency with right loin pain and has an ultrasound performed (Figure A).
- What does this ultrasound show?
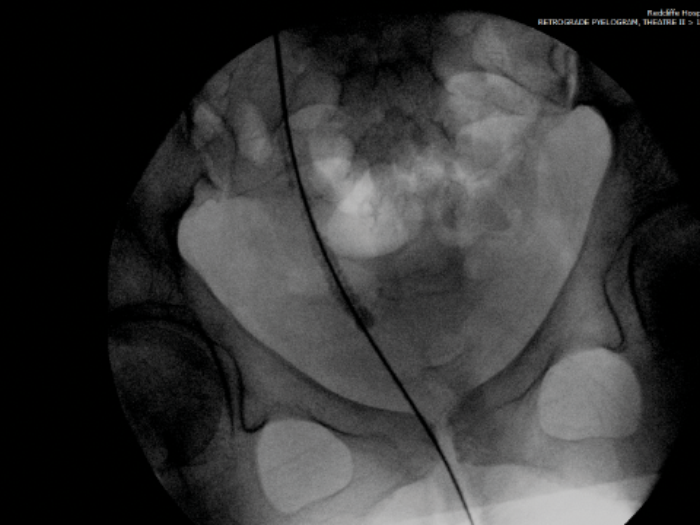
- She is taken to theatre and the intraoperative fluoroscopy is shown (Figure B). What does she have?
- Where does its name come from?

A.
B.
Case 3
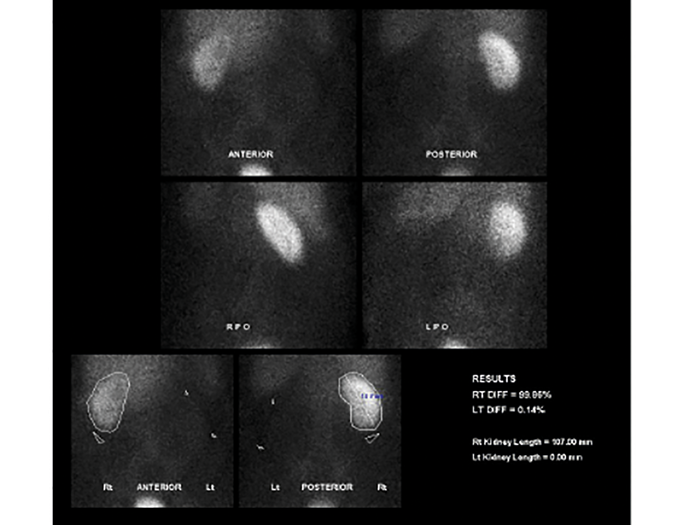
A 74 year old women presents with non-specific abdominal pain and has a plain X-ray KUB taken (Figure A). Subsequently the admitting team arrange a renogram (Figure B)
- What does the KUB x-ray and renogram show?
- What is the likely diagnosis, what is the causative organism and how often is the urinary tract involved?
- How does this infection commonly affect the urinary tract?
- How is it diagnosed?

A.
B.
Case 4
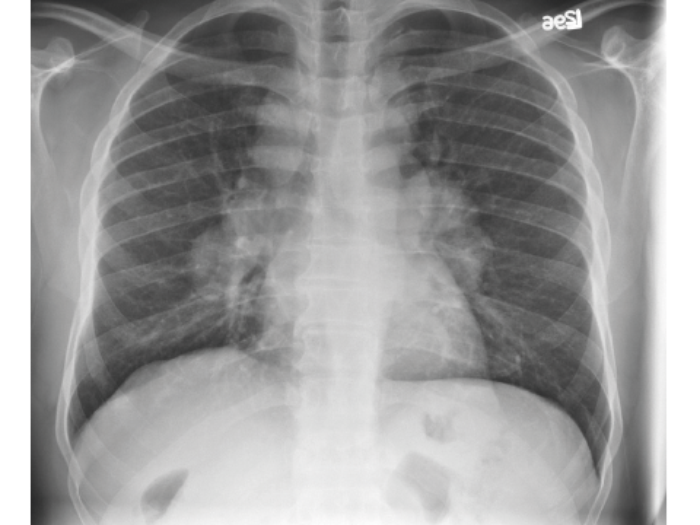
A patient with known nephrocalcinosis has a routine chest radiograph taken for shortness of breath.
- What does this chest radiograph show?
- What is the likely diagnosis?
- Why and how does this condition affect the kidneys?
- How can a diagnosis be established?
Nephrocalcinosis – answers
Case 1
- Multiple areas of small calcification in both kidneys (nephrocalcinosis). Impacted right distal ureteric stone, with multiple small stones proximal to this.
- Causes include: medullary sponge kidney, hypercalcaemia / hypercalciuria, primary hyperparathyroidism, sarcoidosis, and loop diuretics.
- Medullary sponge kidney (MSK) is a congenital disorder relating to malformation of the terminal collecting ducts. Features include collecting duct dilatation associated with medullary cysts. The exact inheritance pattern is poorly understood often with family clustering and with some appearing to follow autosomal dominant pattern.
- The incidence of stones in patients with MSK is difficult to assess as the large majority go undiagnosed. In calcium stone formers, 12-20% have MSK and up to 30% of recurrent stone formers under the age of 20 or women have MSK.
- Treatment is only indicated for recurrent stone formation. The predominant risk factors in MSK are hypercalciuria and hypocitraturia. Potassium citrate therapy is associated with a significant reduction in stone formation in such patients.
- Long-term prognosis in MSK is good. However, occasionally recurrent / chronic stone obstruction can lead to chronic kidney disease.
Case 2
-
Right hydroureter and hydronephrosis. Calcification with medullary shadowing. |
-
Right ureteric steinstrasse.
-
Steinstrasse is German for ‘stone street’. The term was coined by Egbert Schmiedt and Christian Chaussy, German pioneers of shockwave lithotripsy (SWL), in the 1980s. It is often seen as a complication post SWL where stone fragments block the ureter to form a ‘stone street’.
Case 3
-
X-ray: amorphous dystrophic calcification (putty kidney) representing calcified caeseous tissue. Previous spinal stabilisation surgery and metalwork. Renogram: complete loss of function of the left kidney.
-
Renal tuberculosis commonly caused by mycobacterium tuberculosis bacilli; genitourinary TB accounts for 15-20% of extra-pulmonary TB.
-
Papillary necrosis, multifocal strictures, amorphous dystrophic calcification, fibrotic bladder, direct renal and lower urinary tract infections, secondary amyloidosis, adrenal calcification, epididymal mass, epididymorchitis, prostatitis and urethral strictures.
-
Early morning urine (x3) can be sent for acid-fast bacilli cultures. Classic features may be seen on imaging (as in this case) or a positive QuantiFERON blood test (cannot differentiate active or latent disease).
Case 4
-
Bilateral hilar lymphadenopathy.
-
When in association with nephrocalcinosis, sarcoidosis is the likely diagnosis.
-
Sarcoidosis causes abnormalities with calcium metabolism, with extrarenal production of calcitriol by activated macrophages. Manifestations of this include hypercalciuria (up to 50%), hypercalcaemia (10-20%), nephrocalcinosis and nephrolithiasis. If untreated this can lead to chronic renal failure.
-
The diagnosis requires three elements:
-
Compatible clinical and radiographic manifestations (ACElevel, bihilar lymphadenopathy).
-
Exclusion of other similarly presenting diseases.
-
Histopathology displaying non-caeseating granuloma.



