Case 1
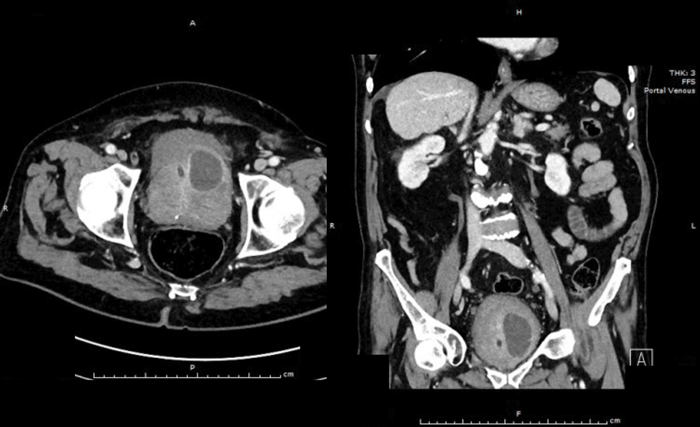
A 76-year-old diabetic man with a long-term catheter presents to the Emergency Department with rigors and non-specific abdominal pain. He has an elevated white cell count (WCC) and C-reactive protein (CRP). An abdominal and pelvic CT scan was arranged. Selected CT images are shown below:
- Describe the CT findings. What is the diagnosis?
- What are potential risk factors in its development?
- Describe the classical clinical findings and appropriate initial investigations.
- How can it be drained?
- What is the most likely causative organism?
- What are the four classifications of prostatitis based on the NIH consensus?
Case 2
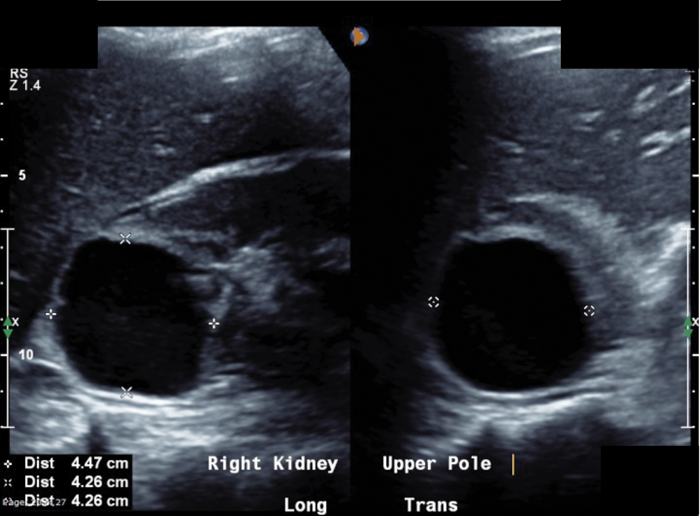
A 34-year-old lady is referred from the medics with right-sided loin pain and urosepsis. An initial ultrasound scan was arranged, followed by a subsequent CT scan. These scans did not show any renal / ureteric stone, but selected images are shown to the left.
- What do the images show?
- What could have happened to cause her symptoms?
- How would you manage her acutely?
- Subsequent microbiology was positive for E.coli. What would be her ongoing management?
Case 3
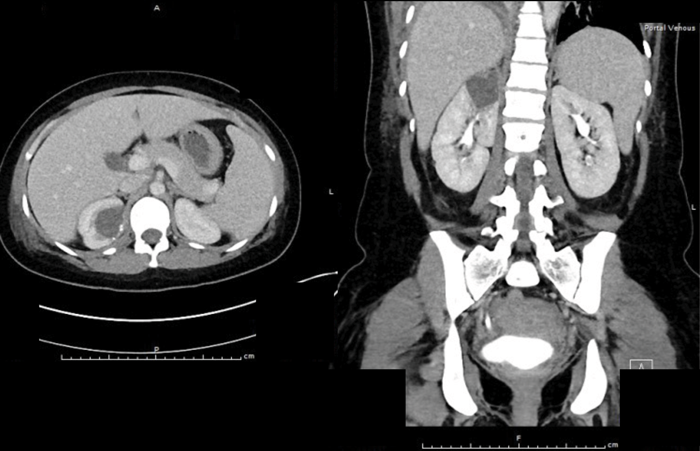
A previously fit and well 65-year-old man presents with acute onset, left loin pain and non-visible haematuria. He underwent a CT KUB suspecting renal stones (no stones seen), therefore he had a subsequent contrast CT scan. These images are shown below:

- What do the contrast CT images show?
- Describe normal renal arterial anatomy.
- What are the common causes of these findings? List a few rarer causes.
- What investigations are needed?
- What are the acute treatment options? 6. What it is the long-term prognosis for the kidney?
Answers
Case 1
-
There is a peripherally enhancing collection in the left antero-superior aspect of the prostate extending into the bladder base, approximately 40mm x 30mm. Diagnosis: left-sided prostatic abscess.
-
UTI, urethral strictures, post urethral instrumentation, bladder catheterisation, prostate biopsy, trauma, immunosuppression, acute bacterial prostatitis.
-
An oedematous and tender prostate on DRE suggests a diagnosis of acute bacterial prostatitis. A trans-rectal ultrasound may show hypoechoic or anechoic areas with a thickened or oedematous wall. CT findings include a non-enhancing fluid density collection that can be multi-septate or rim enhancing.
-
Transurethral (selective TURP over abscess) or perineal aspiration and drainage under radiological guidance.
-
E.coli (up to 80%), other enterobacteriaceae (Klebsiella, Enterobacter and Serratia species) (3-11%), Proteus species (5%), Pseudomonas aeruginosa (5%).
-
I. Acute bacterial prostatitis
II. Chronic bacterial prostatitis
III. Chronic prostatitis/CPPS:
a. Inflammatory
b. Non-inflammatory
IV. Asymptomatic inflammatory prostatitis.
Case 2
-
A well-defined cystic structure in the upper pole of the right kidney. The cystic structure had calcification within the wall. CT demonstrated a fluid density mass within the cyst, with an irregular coarse foci of wall calcification. There is a solitary gas locule within the superior aspect of the cyst.
-
An infected cyst or an acute bleed into the cyst.
-
Start broad spectrum antibiotics and arrange drainage of the cyst (send for culture, cytology and creatinine). Antibiotics must be guided via sensitivities; they enter the cyst by diffusion which is more pronounced with lipid-soluble drugs. Ciprofloxacin and levofloxacin achieve therapeutic concentrations within cysts and are active against gram-negative enteric organisms. Aminoglycosides and penicillins frequently do not penetrate cysts.
-
She would need at least four-six weeks antibiotics. If the infection recurs, antibiotics may be continued for two to three months. In cases of an extremely large infected cyst, antibiotic therapy alone may not be sufficient and definitive cyst drainage may be needed.
Case 3
-
There is diffusely marked hypo perfusion throughout the right kidney. The left kidney demonstrates an infarction of the posterior and superior segments of the left kidney.
-
The first branch off the renal artery is the inferior suprarenal artery. The renal artery has five segmental branches. The posterior segmental artery supplies most of the posterior kidney, with the exception of the lower pole. The anterior branches are: superior segmental artery, anterior superior segmental artery, anterior inferior segmental artery, and inferior segmental artery. These arteries branch into interlobar arteries, which travel in a parallel fashion in between the major calyces and then branch further into arcuate arteries.
-
The two main causes of renal infarction are thromboembolic, commonly from a thrombus in the heart or aorta (cardiomyopathy, endocarditis, artificial valve thrombi or AF) and in-situ thrombosis. Less common causes include: hypercoagulable states, sub-therapeutic warfarin dosing, renal artery dissection, aortic dissection (as in this case), trauma, Marfan syndrome, polyarteritis nodosa or idiopathic.
-
Full blood count (FBC), clotting screen, serum creatinine and lactate dehydrogenase (LDH) levels. Urinalysis, urine culture and electrocardiogram (to diagnose AF). Non-contrast and contrast CT imaging. Echocardiogram may be needed if suspect valvular lesion.
-
Anticoagulation with heparin and warfarin if known underlying disease (e.g. atrial fibrillation, left ventricular thrombus, or a hypercoagulable state) to prevent future events. If the main renal artery or segmental branch occlusion is diagnosed early (less than one to two days from symptom onset) and in selected patients with persistent hypertension, percutaneous endovascular therapy (local thrombolysis, thrombectomy, or stent replacement) may be an option. Start antihypertensive therapy if needed with either an ACE inhibitor or angiotensin II receptor blocker.
-
Sixty-one percent of patients have normal renal function (compensatory hypertrophy of contralateral kidney). Thirteen percent have mild and 18% severe renal impairment, 8% need maintenance dialysis. Thirteen percent have repeat thromboembolic event. Eleven percent die during the first month after diagnosis.


