Advances in fertility treatment since in vitro fertilisation was pioneered by Edwards and Steptoe, cumulating in the birth of Louise Brown in 1978, have been nothing short of remarkable [1]. Since then, a myriad of treatments has been developed for both male and female factor infertility, leading to the birth of over 10 million children worldwide [2].
How these treatments are interrogated for their efficacy and effectiveness has also undergone significant change. Often considered the gold standard of evidence, meta-analysis of well-conducted randomised control trials (RCTs) has been used to guide clinicians and inform patient-centred evidence-based healthcare. How these trials are conducted, their reporting, and now a growing area of concern, their integrity, has become the subject of much debate [3].
Despite limited evidence for many interventions for male and female factor infertility, these treatments are still used in clinical practice, nonetheless. This has led to the UK regulator of fertility treatment and research, the Human Fertilisation and Embryology Authority, developing a traffic light system to rate the quality of the evidence behind these ‘add-ons’ although this system itself has been met with some criticism [4].
While not all interventions can be evaluated through an RCT, one such tongue-in-cheek example being the use of parachutes to prevent major trauma when jumping from an aircraft [5], interrogation of interventions for male and female factor infertility through RCTs is growing [6,7]. A move from the paternalistic healthcare model to shared decision making means now more than ever, clinicians need high-quality, robust evidence to help inform patient decision making.
A unique challenge for male infertility trials
Typically, RCTs would involve a cohort of participants receiving an intervention or a placebo / standard care, with a robust and reproducible tool to measure a pre-defined outcome. These outcomes would usually be measured in the participants receiving the intervention. Infertility trials, in particular male infertility trials, are unique however, in that they have up to three potential participants whose clinical outcomes may be influenced by the intervention. These potential participants include a male participant, their female partner and their potential offspring (Figure 1).
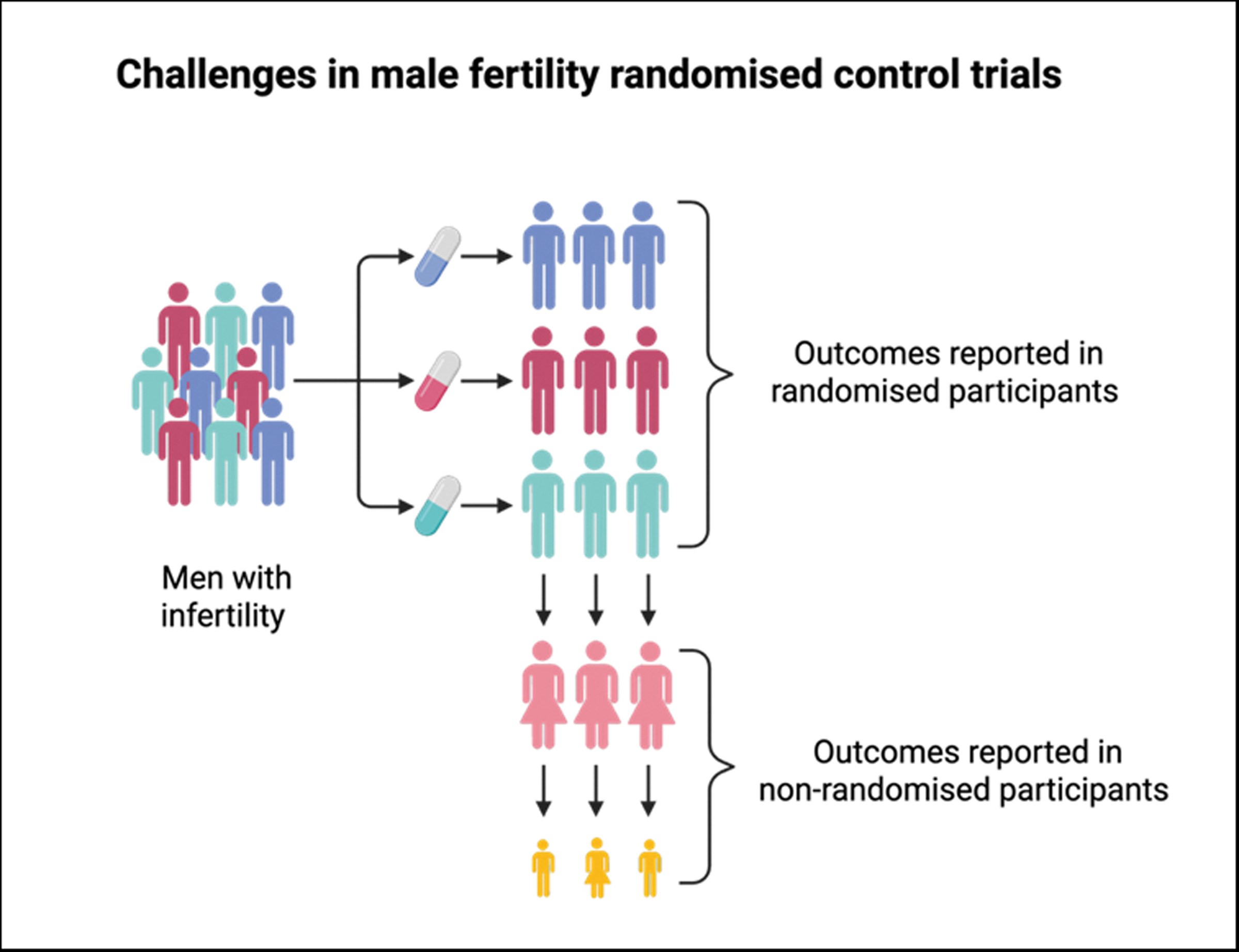
Figure 1: Overview of the challenges in outcome reporting in male fertility randomised control trials, including outcomes in non-randomised participants, influenced by external factors such as aneuploid pregnancy loss.
While male participants will likely be recruited against well-defined criteria and standardised across interventions, their female partners and potential offspring will not. This could lead to substantial and unquantified variations that could impact the outcome of these trials. This is a challenge to identify efficacious interventions for male infertility.
Recent efforts have been developed to address these issues, including priority-setting partnerships, increasing patient participation in the design and implementation of research, and consensus-driven initiatives to identify key outcomes to be collected and reported, referred to as core outcomes, when conducting these trials [8,9].
Inconsistencies in the collection, measurement and reporting of outcomes lead to barriers in synthesising data across trials through meta-analysis. This, in turn, leads to the ongoing use of potentially ineffective and even harmful interventions, further contributing to poor use of limited research funding to conduct further trials to evaluate the efficacy and safety of these interventions [10].
Developing a core outcome set for male fertility trials
A recent systematic review of outcome reporting in the 100 largest randomised control trials in the last 10 years found significant heterogeneity [11]. Some of the examples of this heterogeneity include the nature of the intervention under study, including dietary supplements, surgical interventions and sperm selection techniques. Outcomes reported by these trials also varied with only 47 reporting a clear primary outcome, including semen quality, live birth and pregnancy rate, interestingly defined in 12 different ways or not at all.
While no single initiative can address all the issues encountered when designing and implementing male fertility trials, we can reduce inconsistencies in the outcomes collected and how they are defined and reported. To do this, we have developed a core outcome set for male infertility trials using an internal group of clinicians, researchers and men with lived experiences of infertility. Using a transparent and pre-published methodology to conduct this work, we undertook a two-round Delphi, including 79 outcomes, of which 19 were taken forward for discussion in a consensus development workshop [12]. These can be reviewed in full, as well as the discussion around these in our two published papers [13,14].
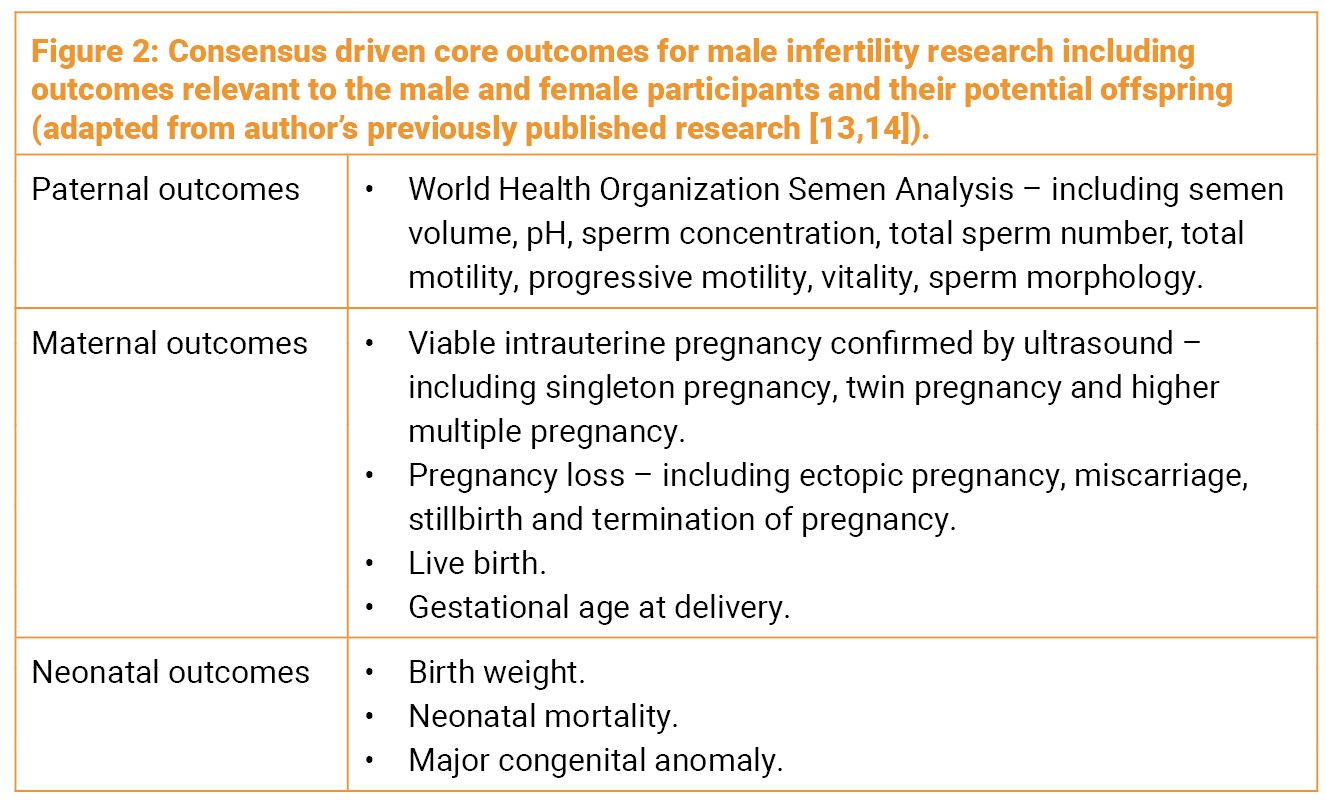
These outcomes are diverse and include outcomes pertinent to both the male and female participants but also their potential offspring (Figure 2) [13,14]. Previous consensus-driven work has been undertaken to establish how these outcomes should be measured and reported, again facilitating the use of this outcome set [15]. By researchers adopting this core outcome set, we hope to standardise the way male fertility trials are conducted and reported to better understand the efficacy and efficiency of these interventions, impacting the care we give to men and their future families.
Take home messages
-
There is significant heterogeneity in the way new interventions for male factor infertility are evaluated.
-
The design and conduct of randomised control trials vary significantly, which is a barrier to meta-analysis of these studies to inform patient care.
-
A core outcome set for male infertility trials has been developed to overcome the inconsistent outcome reporting identified in these studies.
-
This will lead to reduced research waste and facilitate the use of evidence-based interventions for male factor infertility.
References
1. Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet 1978;2:366.
2. Adamson GD, Creighton P, de Mouzon J, et al. How many infants have been born with the help of assisted reproductive technology? Fertil Steril 2025;124(1):40–50..
3. Li W, van Wely M, Gurrin L, Mol BW. Integrity of randomized controlled trials: challenges and solutions. Fertil Steril 2020;113:1113–19.
4. Lensen S, Armstrong S, Vaughan E, et al. “It all depends on why it’s red”: qualitative interviews exploring patient and professional views of a traffic light system for IVF add-ons. Reprod Fertil 2023;4(2):e220136.
5. Yeh RW, Valsdottir LR, Yeh MW, et al. Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial. BMJ 2018;363:k5094.
6. Halpern JA, Brannigan RE. Barriers, potential solutions, and alternatives to randomized clinical trials in male reproductive medicine. Fertil Steril 2019;111:871–2.
7. Wilkinson J, Brison DR, Duffy JMN, et al. Don’t abandon RCTs in IVF. We don’t even understand them. Hum Reprod 2019;34(11):2093–8.
8. Duffy JMN, Adamson GD, Benson E, et al. Top 10 priorities for future infertility research: an international consensus development study. Fertil Steril 2021;115(1):180–90.
9. Graham L, Illingworth B, Showell M, et al. Research priority setting in women’s health: a systematic review. BJOG 2020;127(6):694–700.
10. Chalmers I, Glasziou P. Avoidable waste in the production and reporting of research evidence. Lancet 2009;374:86–9.
11. Rimmer MP, Howie RA, Subramanian V, et al. Outcome reporting across randomised controlled trials evaluating potential treatments for male infertility: a systematic review. Hum Reprod Open 2022;2022(2):hoac010.
12. Rimmer MP, Howie RA, Anderson RA, et al. Protocol for developing a core outcome set for male infertility research: an international consensus development study. Hum Reprod Open 2022;2022(2):hoac014.
13. Rimmer MP, Howie, R, Anderson RA, et al. A core outcome set for future male infertility research: development of an international consensus. Human Reprod. 2025;40:(865-875).
14. Rimmer MP, Howie, R, Anderson RA, et al. A core outcome set for future male infertility research: development of an international consensus. Fertil Steril 2025;123(6):1017–28..
15. Duffy JMN, Bhattacharya S, Bhattacharya S, et al. Standardizing definitions and reporting guidelines for the infertility core outcome set: an international consensus development study. Hum Reprod 2021;115(1):201–12.
Declaration of competing interests: None declared.





