Radical surgical treatment of prostate cancer has become minimally invasive owing to robotic assisted laparoscopic technology [1]. Patients who undergo robotic assisted radical prostatectomy (RARP) often have lower risk of morbidity compared to an open approach. However, patients with a narrow pelvis and a protuberant pubic symphysis can present difficulties in visualising the prostatic apex. This forces some surgeons to consider steps such as pubic symphysiotomy, with a balanced risk of osteitis pubis or osteomyelitis being possible sequelae.
We present a case of a patient who underwent RARP and was subsequently reported to have osteomyelitis on imaging two months after surgery.
Case report
A 70-year-old male of white ethnicity had been diagnosed with unfavourable intermediate risk prostate cancer on a background of his GP checking his prostate specific antigen (PSA), which was 9.8, as part of a routine health check. He was deemed to have an excellent performance status, with a body mass index of 24. He had no pre-existing lower urinary tract symptoms nor history of previous abdominal surgery. Since his MRI (Figure 1a and 1b) staged him as T3a N0, along with Gleason 4+3 prostate acinar adenocarcinoma, he underwent a prostate-specific membrane antigen (PSMA) PET staging scan. This scan confirmed organ confined prostate cancer. The patient elected to undergo a RARP which took place four months after his transperineal prostate biopsy.
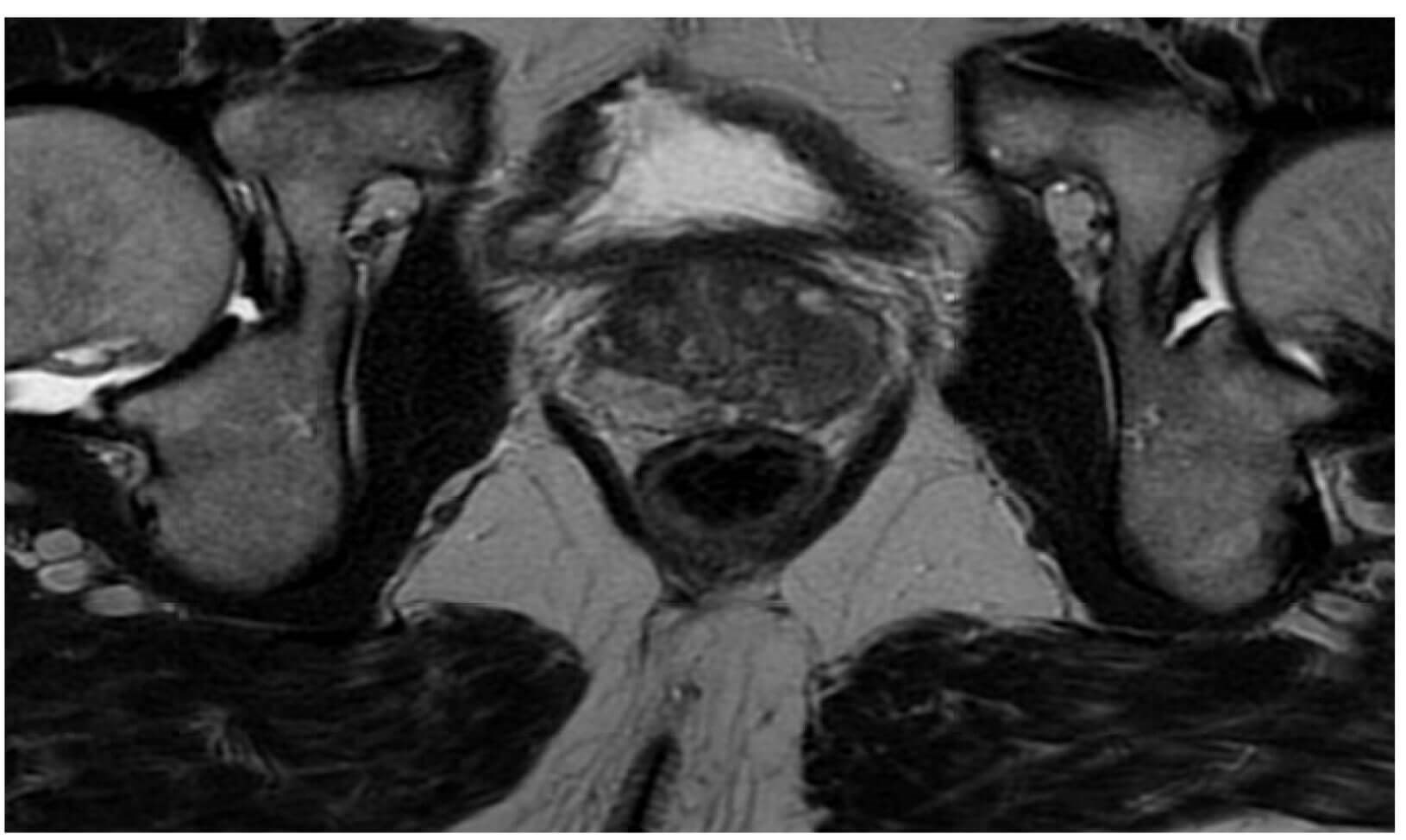
Figure 1a: Pre prostate biopsy MRI pelvis. T2 sequence showing anatomy of the prostate.
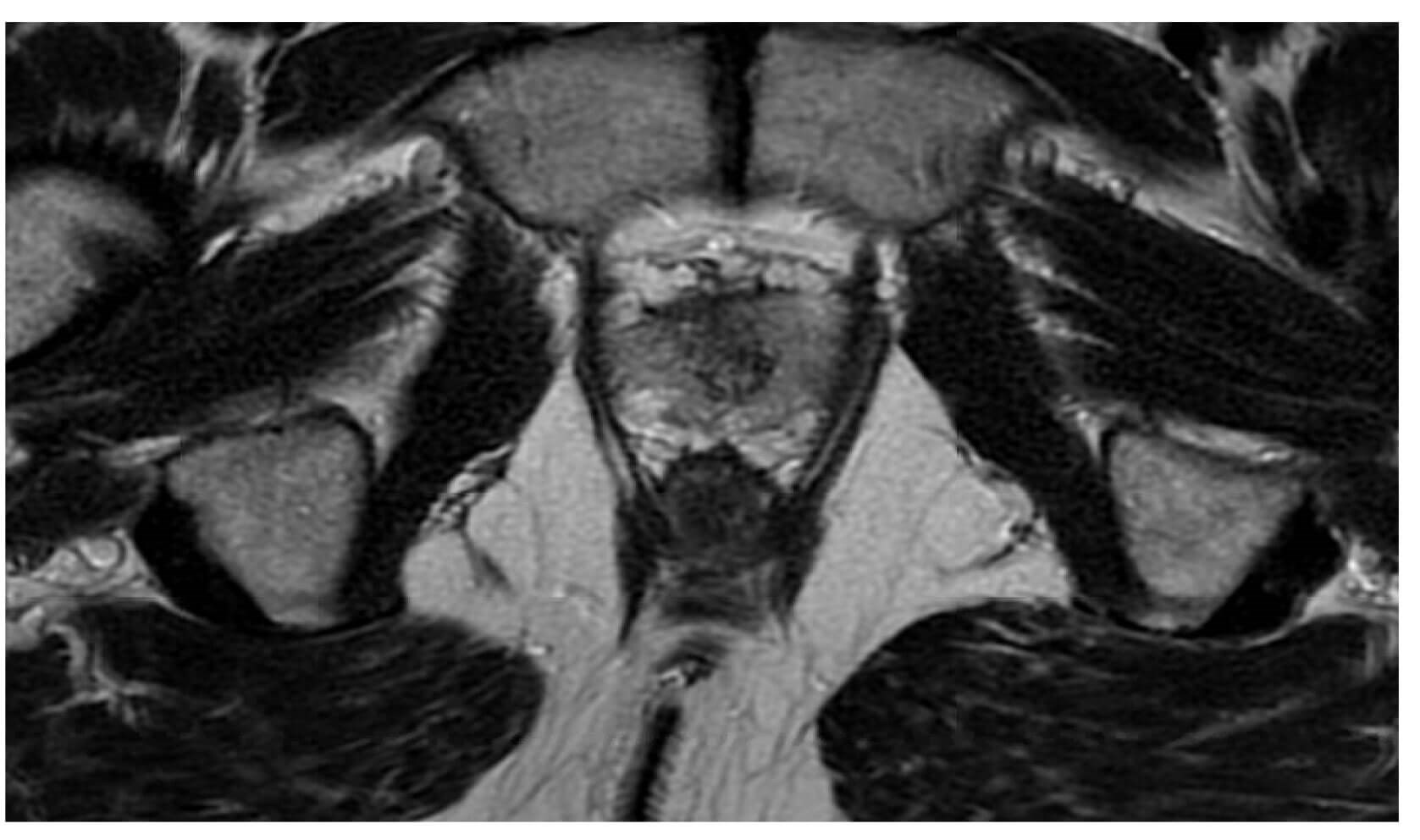
Figure 1b: Pre prostate biopsy MRI pelvis. T2 sequence showing anatomy of the pubic symphysis.
The performing surgeon utilised a standard retropubic transperitoneal robotic approach with a da Vinci system. The pubic symphysis was deemed not to hinder the view of the prostatic apex and so was not shaved nor altered. The operation concluded in just under three hours and the patient had an uneventful hospital stay. He was discharged on postoperative day one. His trial without catheter was 11 days after RARP, without a cystogram. The patient was making good progress until postoperative day 42, when he developed symptoms of a urinary tract infection, along with severe pain in his right groin which limited his mobility. An inguinal hernia was excluded on examination and a urine culture was performed. The urine culture grew Klebsiella, and this along with his musculoskeletal symptoms was managed with outpatient antibiotics and analgesia.
Days after a treatment course was completed for the above UTI, the patient’s groin symptoms became intolerable, and he was admitted to hospital for management. A CT scan was performed to rule out a pelvic collection, and a flexible cystoscopy was performed followed by bladder catheterisation. The cystogram showed no leak, but the CT scan suggested osteomyelitis (Figure 2a). An MRI pelvis (Figure 2b) was requested in order to confirm or refute the presumptive diagnosis made on CT. The MRI report concluded that changes seen in the bone were that of infective osteitis pubis and osteomyelitis. There was also an associated small amount of enhancing fluid at pubic symphysis posteriorly along with mild oedema of right obturator muscles.

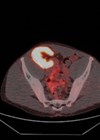
Figure 2a: Post RARP CT image showing loss of articular surfaces of pubic symphysis. No collection.
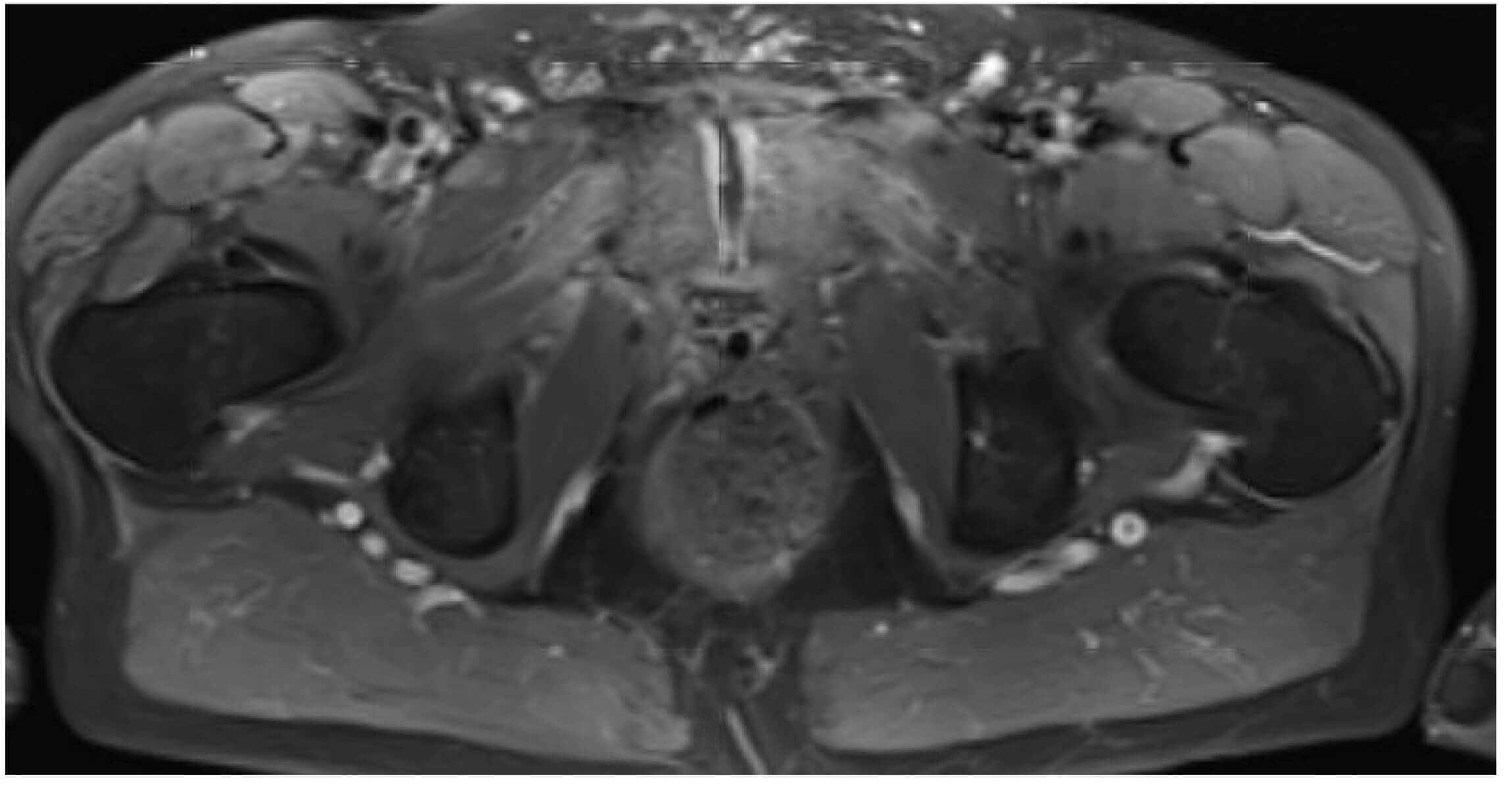
Figure 2b: Post RARP MRI T1 post contrast showing bone marrow signal change and
enhancement around the pubic symphysis. Oedema of the right obturator muscles.
The patient clinically improved with non-steroidal anti-inflammatory medication and physiotherapy. Blood and urine cultures were collected again, while he was not on antibiotics, given that he was systematically well. These second set of cultures grew no organisms and his inflammatory blood markers steadily fell to normal ranges from initially being mildly raised. The advice from the orthopaedic team was to treat conservatively, rather than proceed to a bone biopsy. The patient remains out of hospital, recovering well and is able to increase his mobility now. An interval MRI scan and review in the orthopaedic team’s clinic is scheduled, and uro-oncology clinic thereafter.
His prostate histopathology assessment showed Gleason score 4+3=7 with negative margins, pathological stage pT2 and a recent PSA of <0.01ug/L.
Discussion
The increased utilisation of robotic surgery has allowed standardisation of operative steps and has changed a previously major open pelvic procedure to one that can be performed as a day case in select cases [2]. During open surgery, it is recognised that the posterior symphysis can be prominent and obscure the prostate apex, which is particularly challenging in black patients who are known to have distinctly narrow and steep access to their prostate. It is a combination of posterior symphysis being protuberant (which can happen in any ethnicity) that presents an additional challenge for these patients undergoing prostatectomy. Superficial electrocautery resection of this prominence is one mainstay manoeuvre, along with increased flexion of the table during an open approach [3].
The robotic approach enables this with use of minimally invasive cameras with x10 magnification, but this manoeuvre can also be achieved using monopolar scissors at the surgeon’s discretion.
Osteomyelitis pubis vs. osteitis pubis
The pubic symphysis is similar to sacroiliac and intervertebral joints in that they are amphiarthroidal with limited mobility. During foetal development, the thickened cartilaginous endplates can become thin as we mature [4]. Muscles that are responsible for hip and thigh movement have their origin from the pubic bone inferiorly and the pelvic floor muscles insert posteriorly.
Osteitis pubis has a non-infective aetiology, with its occurrence commonly in athletes due to stress on the joint. Football players seem particularly prone to this, as supported by a radiographical study that examined them compared to non-athletes. The former group was likely to have findings of bony irregularity and reactive sclerosis of the pubic symphysis [5]. This condition is usually self-limiting and responds to anti-inflammatory medication and rest.
In contrast, osteomyelitis pubis is an infectious process that can present similarly to osteitis pubis. A study of 100 cases in several clinical and surgical scenarios found variability in serum inflammatory marker response with blood cultures were positive in 73% of cases. However, a culture of a needle aspirate of the symphysis pubis had the highest sensitivity [6]. Management is an extended intravenous antibiotic course and, in some cases, surgical debridement.
Urological causes of pubic symphysis conundrum
According to a recent literature review [7], procedures in urology that have been complicated by osteitis pubis are urethropexy, transurethral prostate surgery (electrosurgical or laser), focal therapy energy to manage prostate cancer, radiotherapy and radical prostatectomy or cystectomy.
A sinus formation from the prostate capsule to the pubic bone along with an infected urinoma can result in inflammatory process. MRI imaging is a sensitive tool in demonstrating a sinus [8], but is also the gold standard in the diagnosis of acute versus chronic osteitis pubis [9].
In the performance of radical prostatectomy or cystectomy, iatrogenic trauma to the pubic bone by instruments for retraction, or by electrocautery can lend itself to these conditions.
Conclusion
The literature on osteomyelitis pubis and osteitis pubis after RARP is scarce, and this case aims to inform the urologic readership that delayed severe groin pain should focus the investigations to rule these out.
The patient has recovered his urinary continence and will continue his potency rehabilitation. The pelvic surgery team will work to address how these two similar conditions with differing management, can be anticipated and prevented in future urologic procedures.
References
1. https://www.npca.org.uk/content/
uploads/2022/01/NPCA-Annual-Report
-2021_Final_13.01.22-1.pdf
[accessed 6 December 2022].
2. Reddy SS, Noël J, Covas Moschovas M, et al. Same-day discharge protocol for robot-assisted radical prostatectomy: experience of a high-volume referral center. J Endourol 2022;36(7):934-40.
3. Aiken WD, Chin W. Surgical access for radical retropubic prostatectomy in the phenotypically narrow and steep black male’s pelvis is exacerbated by a posterior pubic symphyseal protuberance: A case report. International Journal of Surgery Case Reports 2015;13:88-90.
4. Gamble JG, Simmons SC, Freedman M. The symphysis pubis. Anatomic and pathologic considerations. Clin Orthop Relat Res 1986;(203):261-72.
5. Harris NH, Murray RO. Lesions of the symphysis in athletes. Br Med J 1974;4(5938):211-14.
6. Ross JJ, Hu LT. Septic arthritis of the pubic symphysis: review of 100 cases. Medicine (Baltimore) 2003;82(5):340-5.
7. Amer ML, Omar K, Malde S, et al. The challenges in diagnosis and management of osteitis pubis: An algorithm based on current evidence. BJUI Compass 2022;3(4):267-76.
8. Ziesel C, Frees S, Thomas C, et al. Pubic symphysitis after transurethral resection of the prostate. World J Urol 2016;34:275-80.
9. Gomella P, Mufarrij P. Osteitis pubis: A rare cause of suprapubic pain. Rev Urol 2017;19:156-63.